

Clinicopathologic features and prognosis of epithelioid glioblastoma
- PMID: 32782671
- PMCID: PMC7414508
Clinicopathologic features and prognosis of epithelioid glioblastoma
Abstract
Objective: To improve the understanding of epithelioid glioblastoma (E-GBM) and provide accurate basis for clinical diagnosis, treatment, and prognosis through the analysis of clinicopathologic characteristics, immunohistochemical expression, molecular characteristics, and prognosis of E-GBM.
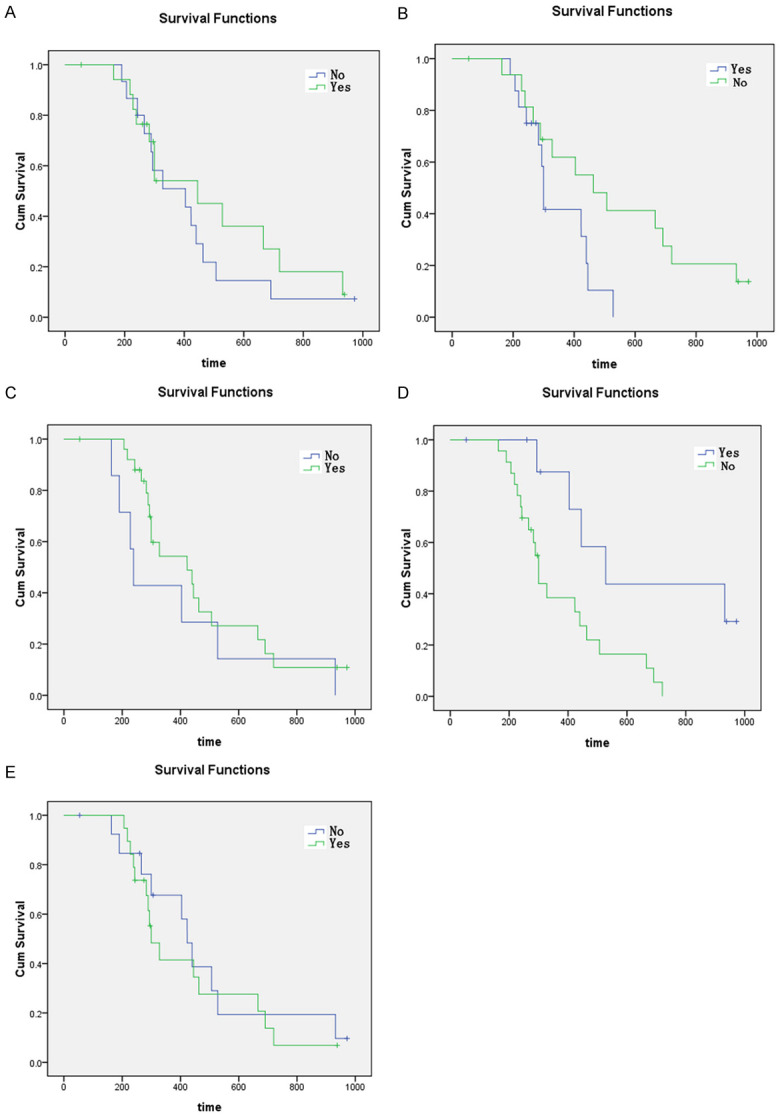
Methods: The clinicopathologic characteristics of 33 cases of E-GBM in our hospital from January 2015 to September 2019 were analyzed retrospectively. Kaplan Meier method was used for survival analysis. Multivariate Cox regression analysis was used to screen the independent risk factors affecting the survival time of patients.
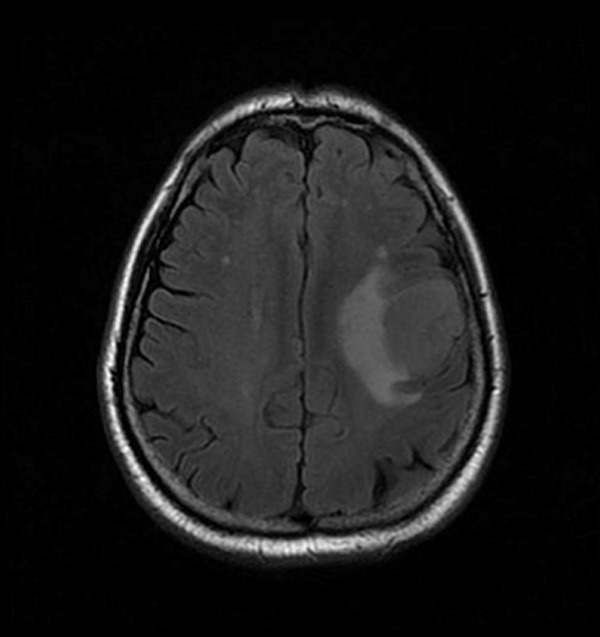
Results: Among 33 patients with E-GBM, 16 were male and 17 were female. The age ranged from 9 to 67 years old, with the median age of 36 years old and the average age of 38 years old. The tumor size (calculated by the largest diameter): 1-6 cm, average size: 3.5 cm. The ratio of smoking and non-smoking is 17:16. All the tumors were located in the cerebral hemisphere, and 26 cases (78.79%) of brain MR showed that the tumors invaded the cortex (white matter).
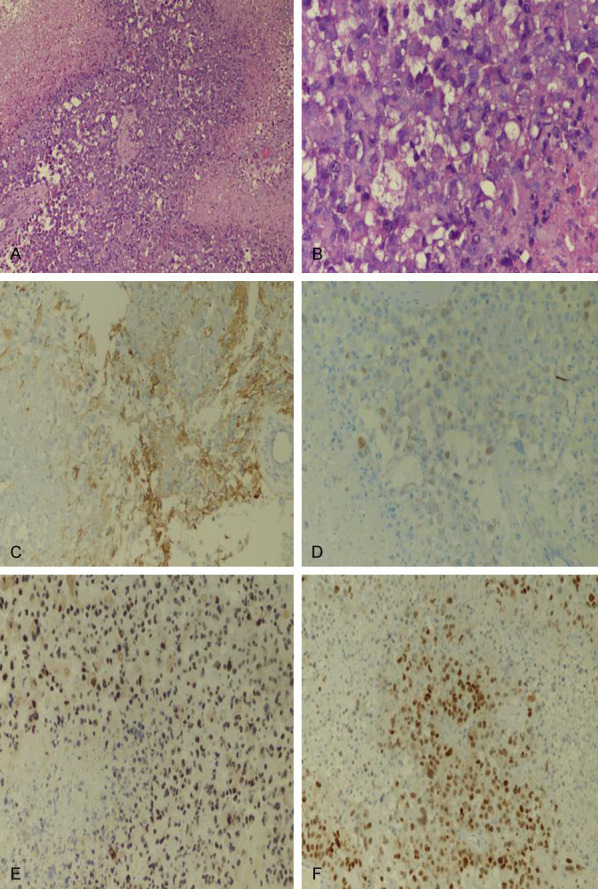
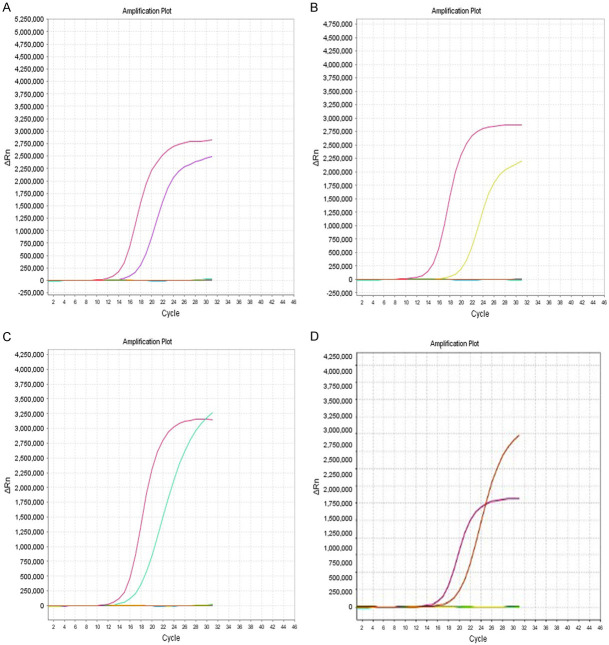
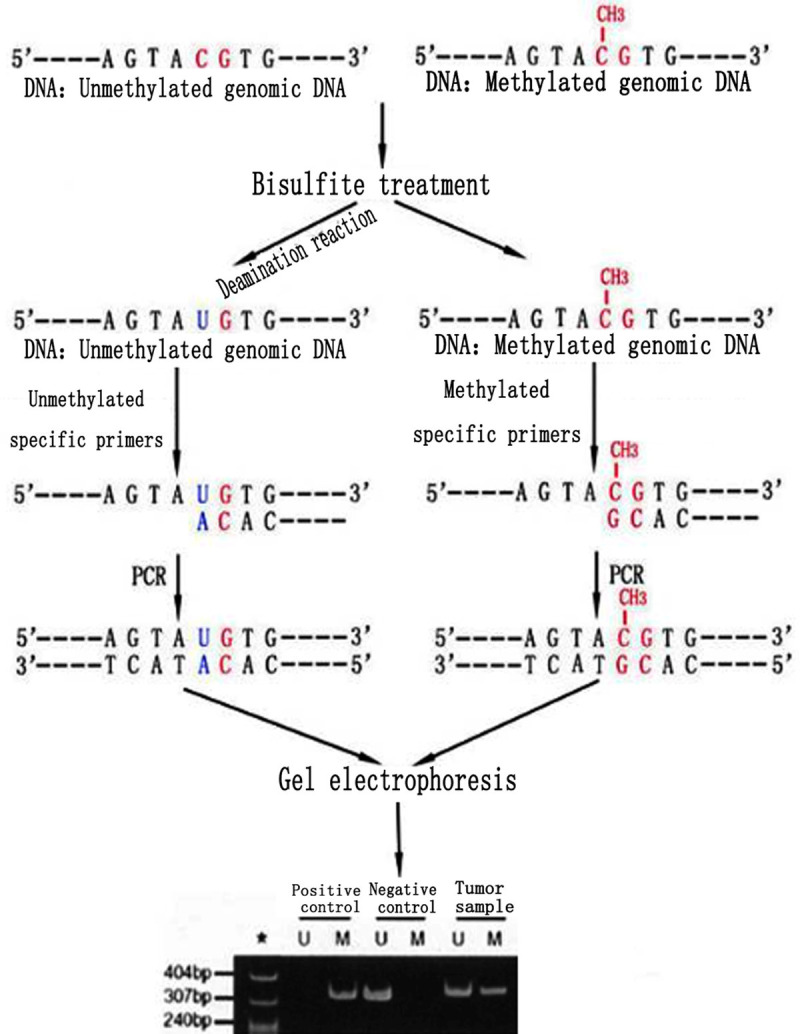
Clinical symptoms: asymptomatic physical examination was found in 6 cases (18.18%), 5 cases (15.15%) had epilepsy history, 2 cases (6.06%) had malignant vomiting, 3 cases (9.09%) had hypertension history, and 17 cases (51.52%) had headache and dizziness. All patients received surgery (total or partial resection). Postoperative radiotherapy was given in 7 cases (21.00%), chemotherapy (TMZ temozolomide) in 3 cases (1.00%), and combined chemoradiotherapy in 16 cases (48.40%). Immunohistochemical staining: the positive rates of CK, GFAP, IDH-1, IDH-2, HMB45, Desmin, BRAF, P53, ATRX, INI-1, S-100, Ki-67 were 20/33, 30/33, 1/33, 1/33, 0/33, 0/33, 33/33, 5/33, 30/33, 33/33, 6/33, Ki-67 of all cases were higher than 40%, among which 11 cases were higher than 60%. The detection of related genes showed that 33 cases (100%) had BRAF V600E mutation. TERT mutation was found in 18 cases (54.5%); IDH1 mutation was found in 1 case (3%); MGMT promoter methylation was found in 15 cases (45.4%); EGFR amplification and 1p/19q co-deletion were not found in any cases.
Conclusion: E-GBM is a highly invasive and rare malignant nervous system tumor, with poor prognosis and lack of clinical specificity. Immunohistochemically, the higher expression of CK, GFAP and Ki67 proliferation index is more conducive to the diagnosis and differential diagnosis of E-GBM. Smoking, brain MR showing tumor invasion of cortex, TERT mutation, radiotherapy, and chemotherapy are independent risk factors affecting the prognosis (survival time) of patients.
Keywords: Cox analysis; Epithelioid; clinical pathology; glioblastoma; prognosis.
IJCEP Copyright © 2020.
Conflict of interest statement
None.
Figures
References
-
- Kepes JJ, Fulling KH, Garcia JH. The clinical significance of “adenoid” formations of neoplastic astrocytes, imitating metastatic carcinoma, in gliosarcomas. A review of five cases. Clin Neuropathol. 1982;1:139–50. - PubMed
-
- Malzkorn B, Reifenberger G. Practical implications of integrated glioma classification according to the World Health Organization classification of tumors of the central nervous system 2016. Curr Opin Oncol. 2016;28:494–501. - PubMed
-
- Korshunov A, Chavez L, Sharma T, Ryzhova M, Schrimpf D, Stichel D, Capper D, Sturm D, Kool M, Habel A, Kleinschmidt-DeMasters BK, Rosenblum M, Absalyamova O, Golanov A, Lichter P, Pfister SM, Jones DTW, Perry A, von Deimling A. Epithelioid glioblastomas stratify into established diagnostic subsets upon integrated molecular analysis. Brain Pathol. 2018;28:656–662. - PMC - PubMed
-
- Alexandrescu S, Korshunov A, Lai SH, Dabiri S, Patil S, Li R, Shih CS, Bonnin JM, Baker JA, Du E, Scharnhorst DW, Samuel D, Ellison DW, Perry A. Epithelioid glioblastomas and anaplastic epithelioid pleomorphic xanthoastrocytomas--same entity or first cousins? Brain Pathol. 2016;26:215–23. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous