

Analysis of cardiopulmonary findings in COVID-19 fatalities: High incidence of pulmonary artery thrombi and acute suppurative bronchopneumonia
- PMID: 32784110
- PMCID: PMC7365076
- DOI: 10.1016/j.carpath.2020.107263
Analysis of cardiopulmonary findings in COVID-19 fatalities: High incidence of pulmonary artery thrombi and acute suppurative bronchopneumonia
Abstract
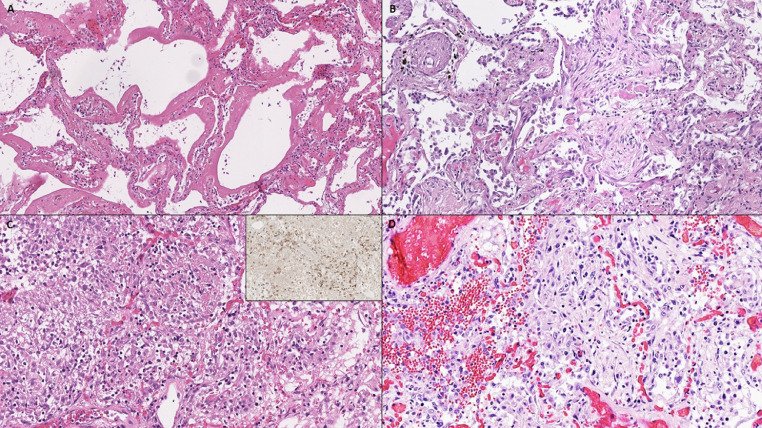
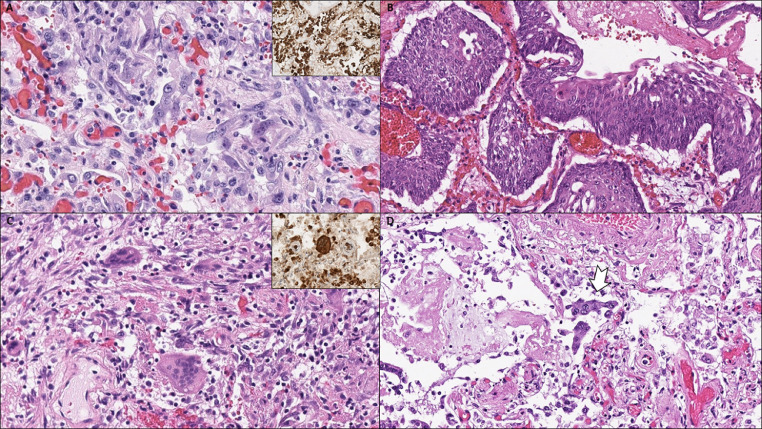
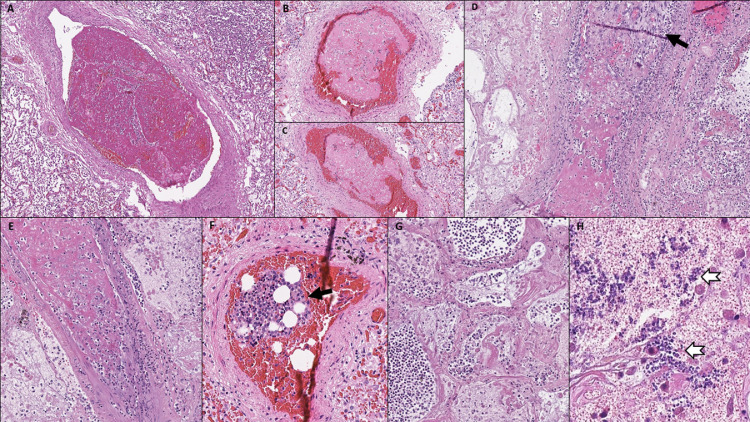
Since its recognition in December 2019, coronavirus disease 2019 (COVID-19) caused by SARS-CoV-2 has rapidly spread globally causing a pandemic that represents the greatest medical challenge in decades. The aim of the study was to evaluate the spectrum of cardiopulmonary pathology of COVID-19 based on (non-minimal invasive) autopsies performed on 14 COVID-19 decedents. Bilateral diffuse alveolar damage (DAD) was found in all patients. Superimposed acute bronchopneumonia was present in 11 of 14 (78.6%) patients and was considered the major cause of death in 2 patients. A key finding was the presence of thrombotic/thromboembolic vascular occlusions. We classified 5 types of pulmonary thrombi: 1. capillary microthrombi (11/14, 78.6%); 2. partially organized thrombi in mid-sized pulmonary arteries with complete vessel occlusion; 3. non-organized thrombi in mid-sized pulmonary arteries that did not completely fill out the vessel lumen and probably represented thromboemboli rather than thrombosis; 4. bone marrow emboli (1/14, 7.1%); and 5. septic pulmonary thromboemboli (1/14, 7.1%). Pulmonary thrombi in mid-sized arteries were noted in 5 of 14 (35.7%) patients, causing pulmonary infarction and/or pulmonary hemorrhage. All patients had evidence of chronic cardiac disease, including myocardial hypertrophy (13/14, 92.9%), mild to marked coronary artery atherosclerosis (14/14, 100%) and focal myocardial fibrosis (3/14, 21.4%). Acute myocardial infarction was found as concurrent cause of death in 3 (21.4%) patients, and significant cardiac hypertrophy (heart weight 750 g) was present in 1 (7.1%) patient with ATTR-positive cardiac amyloidosis. The autopsy findings confirm that COVID-19 is a systemic disease, with major involvement of the lungs, that increases the risk of cardiac and vascular complications including acute myocardial injury and thrombotic/thromboembolic events. Secondary acute bronchopneumonia is a common complication in patients with COVID-19 and may be the major cause of death.
Keywords: Autopsy; COVID-19; Cardiopulmonary pathology; Coronavirus; Diffuse alveolar damage; SARS-CoV-2.
Copyright © 2020. Published by Elsevier Inc.
Figures




Comment in
-
Emerging pulmonary histopathological findings in COVID-19 patients- a letter to the editor in response to Grosse et al. 2020.Cardiovasc Pathol. 2021 Mar-Apr;51:107302. doi: 10.1016/j.carpath.2020.107302. Epub 2020 Nov 3. Cardiovasc Pathol. 2021. PMID: 33152459 Free PMC article. No abstract available.
References
-
- Johns Hopkins University&Medicine. COVID-19 dashboard by the Center for Systems Science and Engineering (CSSE). Available at: https://coronavirus.jhu.edu/map.html; Accessed July 6, 2020.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
