

Evolution of Urothelial Bladder Cancer in the Context of Molecular Classifications
- PMID: 32784716
- PMCID: PMC7461199
- DOI: 10.3390/ijms21165670
Evolution of Urothelial Bladder Cancer in the Context of Molecular Classifications
Abstract
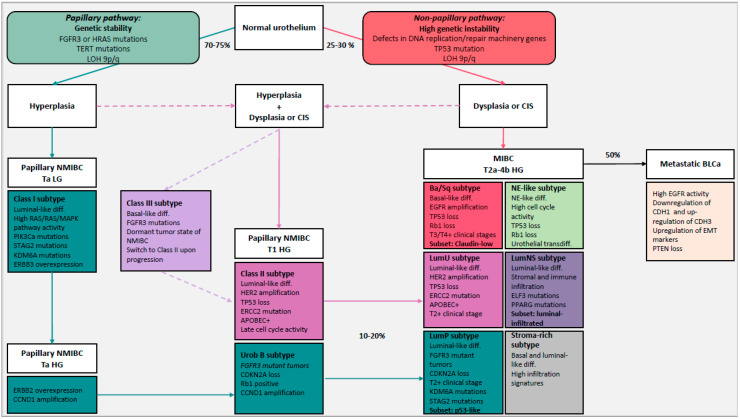
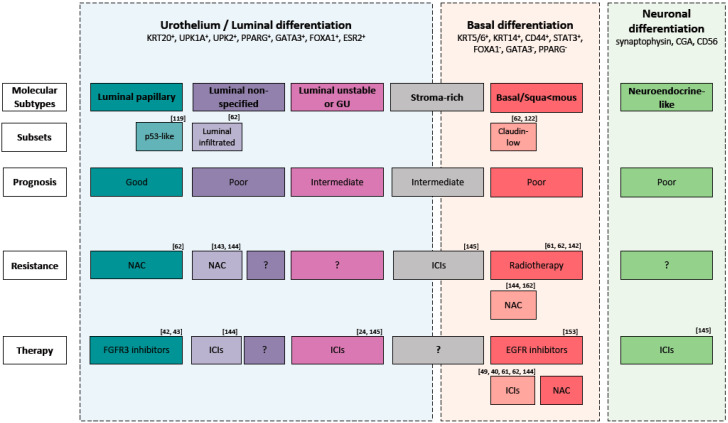
Bladder cancer is a heterogeneous disease that is not depicted by current classification systems. It was originally classified into non-muscle invasive and muscle invasive. However, clinically and genetically variable tumors are summarized within both classes. A definition of three groups may better account for the divergence in prognosis and probably also choice of treatment. The first group represents mostly non-invasive tumors that reoccur but do not progress. Contrarily, the second group represent non-muscle invasive tumors that likely progress to the third group, the muscle invasive tumors. High throughput tumor profiling improved our understanding of the biology of bladder cancer. It allows the identification of molecular subtypes, at least three for non-muscle invasive bladder cancer (Class I, Class II and Class III) and six for muscle-invasive bladder cancer (luminal papillary, luminal non-specified, luminal unstable, stroma-rich, basal/squamous and neuroendocrine-like) with distinct clinical and molecular phenotypes. Molecular subtypes can be potentially used to predict the response to treatment (e.g., neoadjuvant chemotherapy and immune checkpoint inhibitors). Moreover, they may allow to characterize the evolution of bladder cancer through different pathways. However, to move towards precision medicine, the understanding of the biological meaning of these molecular subtypes and differences in the composition of cell subpopulations will be mandatory.
Keywords: bladder cancer; classification; evolution; molecular subtypes; muscle invasive; non-muscle invasive; targeted therapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
