

Virtual Reality, Augmented Reality, Gamification, and Telerehabilitation: Psychological Impact on Orthopedic Patients' Rehabilitation
- PMID: 32784745
- PMCID: PMC7465609
- DOI: 10.3390/jcm9082567
Virtual Reality, Augmented Reality, Gamification, and Telerehabilitation: Psychological Impact on Orthopedic Patients' Rehabilitation
Abstract
Background: Remote virtual rehabilitation aroused growing interest in the last decades, and its role has gained importance following the recent spread of COVID19 pandemic. The advantages of virtual reality (VR), augmented reality (AR), gamification, and telerehabilitation have been demonstrated in several medical fields. In this review, we searched the literature for studies using these technologies for orthopedic rehabilitation and analyzed studies' quality, type and field of rehabilitation, patients' characteristics, and outcomes to describe the state of the art of VR, AR, gamification, and telerehabilitation for orthopedic rehabilitation.
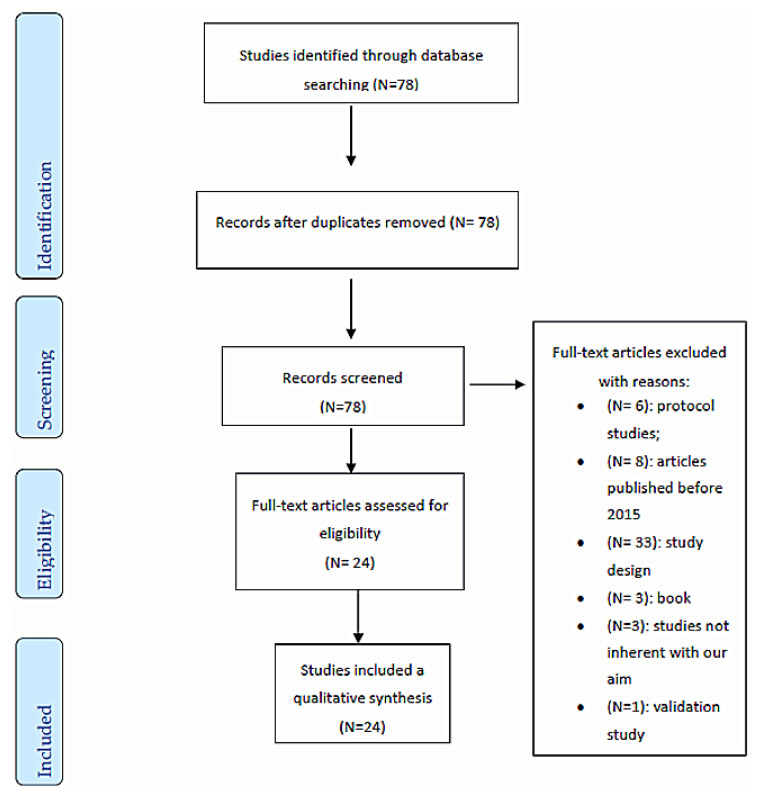
Methods: A comprehensive search on PubMed, Medline, Cochrane, CINAHL, and Embase databases was conducted. This review was performed according to PRISMA guidelines. Studies published between 2015 and 2020 about remote virtual rehabilitations for orthopedic patients were selected. The Methodological Index for Non-Randomized Studies (MINORS) and Cochrane Risk-of-Bias assessment tool were used for quality assessment.
Results: 24 studies (9 randomized controlled trials (RCTs) and 15 non-randomized studies) and 2472 patients were included. Studies mainly concern telerehabilitation (56%), and to a lesser extent VR (28%), AR (28%), and gamification (16%). Remote virtual technologies were used following knee and hip arthroplasty. The majority of included patients were between 40 and 60 years old and had a university degree. Remote virtual rehabilitation was not inferior to face-to-face therapy, and physical improvements were demonstrated by increased clinical scores. Orthopedic virtual remote rehabilitation decreased costs related to transports, hospitalizations, and readmissions.
Conclusion: The heterogeneity of included studies prevented a meta-analysis of their results. Age and social context influence adaptability to technology, and this can modify compliance to treatment and outcomes. A good relationship between patient and physiotherapist is essential for treatment compliance and new technologies are useful to maintain clinical interactions remotely. Remote virtual technologies allow the delivery of high-quality care at reduced costs. This is a necessity given the growing demand for orthopedic rehabilitation and increasing costs related to it. Future studies need to develop specific and objective methods to evaluate the clinical quality of new technologies and definitively demonstrate advantages of VR, AR, gamification, and telerehabilitation compared to face-to face orthopedic rehabilitation.
Keywords: ankle; augmented reality; elbow; femur; foot; gamification; hand; hip; humerus; knee; orthopedic; physiotherapy; rehabilitation; remote rehabilitation; shoulder; spine; telerehabilitation; virtual reality; virtual rehabilitation; wrist.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Allam A.A., Kostova Z., Nakamoto K., Schulz P.J., Merolli M., Lindsay S., Rini C. The Effect of social support features and gamification on a web-based intervention for rheumatoid arthritis patients: Randomized controlled Trial. J. Med. Internet Res. 2015;17:e14. doi: 10.2196/jmir.3510. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
Research Materials
