

A Randomized, Double-blind, Multicenter Trial Comparing Efficacy and Safety of Imipenem/Cilastatin/Relebactam Versus Piperacillin/Tazobactam in Adults With Hospital-acquired or Ventilator-associated Bacterial Pneumonia (RESTORE-IMI 2 Study)
- PMID: 32785589
- PMCID: PMC8662781
- DOI: 10.1093/cid/ciaa803
A Randomized, Double-blind, Multicenter Trial Comparing Efficacy and Safety of Imipenem/Cilastatin/Relebactam Versus Piperacillin/Tazobactam in Adults With Hospital-acquired or Ventilator-associated Bacterial Pneumonia (RESTORE-IMI 2 Study)
Abstract
Background: Imipenem combined with the β-lactamase inhibitor relebactam has broad antibacterial activity, including against carbapenem-resistant gram-negative pathogens. We evaluated efficacy and safety of imipenem/cilastatin/relebactam in treating hospital-acquired/ventilator-associated bacterial pneumonia (HABP/VABP).
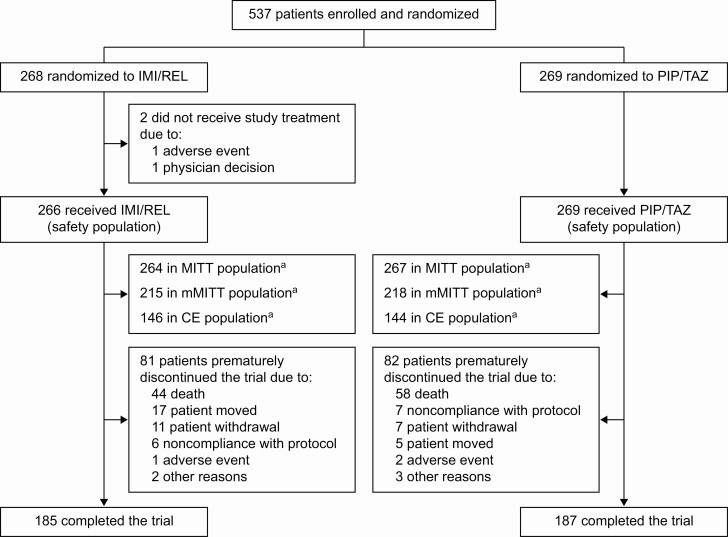
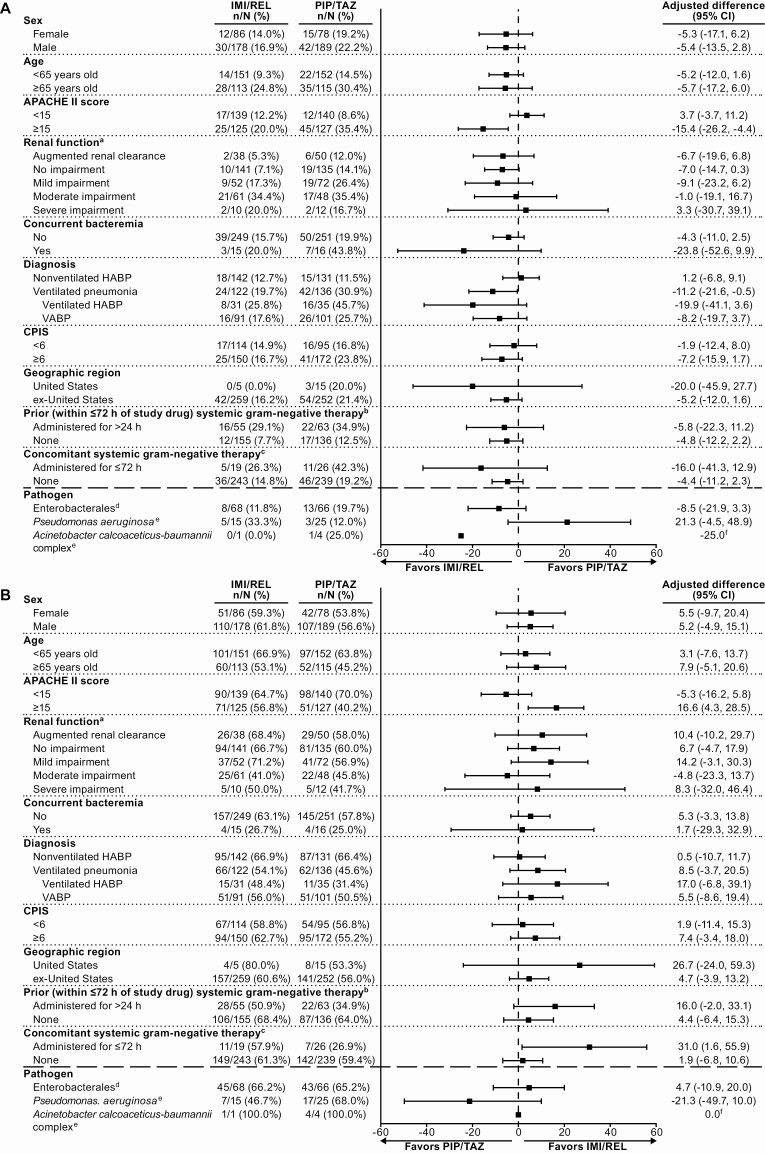
Methods: This was a randomized, controlled, double-blind phase 3 trial. Adults with HABP/VABP were randomized 1:1 to imipenem/cilastatin/relebactam 500 mg/500 mg/250 mg or piperacillin/tazobactam 4 g/500 mg, intravenously every 6 hours for 7-14 days. The primary endpoint was day 28 all-cause mortality in the modified intent-to-treat (MITT) population (patients who received study therapy, excluding those with only gram-positive cocci at baseline). The key secondary endpoint was clinical response 7-14 days after completing therapy in the MITT population.
Results: Of 537 randomized patients (from 113 hospitals in 27 countries), the MITT population comprised 264 imipenem/cilastatin/relebactam and 267 piperacillin/tazobactam patients; 48.6% had ventilated HABP/VABP, 47.5% APACHE II score ≥15, 24.7% moderate/severe renal impairment, 42.9% were ≥65 years old, and 66.1% were in the intensive care unit. The most common baseline pathogens were Klebsiella pneumoniae (25.6%) and Pseudomonas aeruginosa (18.9%). Imipenem/cilastatin/relebactam was noninferior (P < .001) to piperacillin/tazobactam for both endpoints: day 28 all-cause mortality was 15.9% with imipenem/cilastatin/relebactam and 21.3% with piperacillin/tazobactam (difference, -5.3% [95% confidence interval {CI}, -11.9% to 1.2%]), and favorable clinical response at early follow-up was 61.0% and 55.8%, respectively (difference, 5.0% [95% CI, -3.2% to 13.2%]). Serious adverse events (AEs) occurred in 26.7% of imipenem/cilastatin/relebactam and 32.0% of piperacillin/tazobactam patients; AEs leading to treatment discontinuation in 5.6% and 8.2%, respectively; and drug-related AEs (none fatal) in 11.7% and 9.7%, respectively.
Conclusions: Imipenem/cilastatin/relebactam is an appropriate treatment option for gram-negative HABP/VABP, including in critically ill, high-risk patients.
Clinical trials registration: NCT02493764.
Keywords: Pseudomonas; KPC; carbapenem resistant; mechanical ventilation; nosocomial pneumonia.
© The Author(s) 2020. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
Comment in
-
Limitations of Registration Trials for Nosocomial Pneumonia.Clin Infect Dis. 2021 Dec 6;73(11):e4549-e4551. doi: 10.1093/cid/ciaa926. Clin Infect Dis. 2021. PMID: 32785576 No abstract available.
References
-
- Torres A, Niederman MS, Chastre J, et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociacion Latinoamericana del Torax (ALAT). Eur Respir J 2017; 50:1700582. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
