

Prognostic performance of endothelial biomarkers to early predict clinical deterioration of patients with suspected bacterial infection and sepsis admitted to the emergency department
- PMID: 32785865
- PMCID: PMC7423829
- DOI: 10.1186/s13613-020-00729-w
Prognostic performance of endothelial biomarkers to early predict clinical deterioration of patients with suspected bacterial infection and sepsis admitted to the emergency department
Abstract
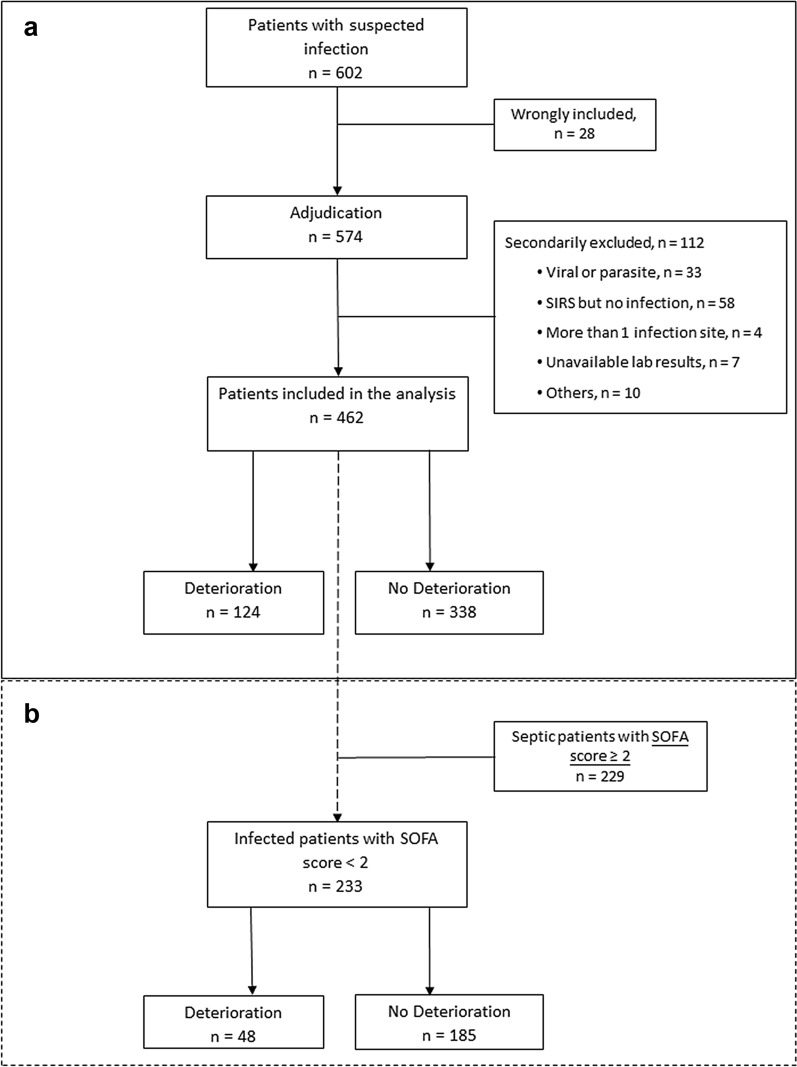
Background: The objective of this study was to evaluate the ability of endothelial biomarkers to early predict clinical deterioration of patients admitted to the emergency department (ED) with a suspected sepsis. This was a prospective, multicentre, international study conducted in EDs. Adult patients with suspected acute bacterial infection and sepsis were enrolled but only those with confirmed infection were analysed. The kinetics of biomarkers and organ dysfunction were collected at T0, T6 and T24 hours after ED admission to assess prognostic performances of sVEGFR2, suPAR and procalcitonin (PCT). The primary outcome was the deterioration within 72 h and was defined as a composite of relevant outcomes such as death, intensive care unit admission and/or SOFA score increase validated by an independent adjudication committee.
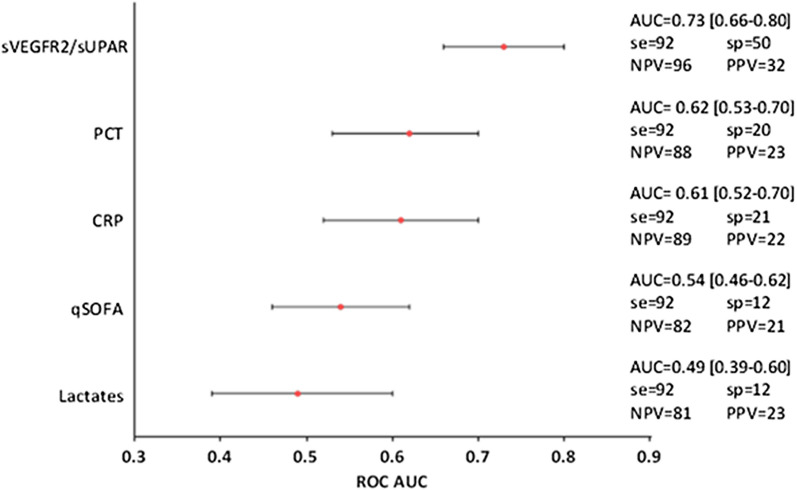
Results: After adjudication of 602 patients, 462 were analysed including 124 who deteriorated (27%). On admission, those who deteriorated were significantly older (73 [60-82] vs 63 [45-78] y-o, p < 0.001) and presented significantly higher SOFA scores (2.15 ± 1.61 vs 1.56 ± 1.40, p = 0.003). At T0, sVEGFR2 (5794 [5026-6788] vs 6681 [5516-8059], p < 0.0001), suPAR (6.04 [4.42-8.85] vs 4.68 [3.50-6.43], p < 0.0001) and PCT (7.8 ± 25.0 vs 5.4 ± 17.9 ng/mL, p = 0.001) were associated with clinical deterioration. In multivariate analysis, low sVEGFR2 expression and high suPAR and PCT levels were significantly associated with early deterioration, independently of confounding parameters (sVEGFR2, OR = 1.53 [1.07-2.23], p < 0.001; suPAR, OR = 1.57 [1.21-2.07], p = 0.003; PCT, OR = 1.10 [1.04-1.17], p = 0.0019). Combination of sVEGFR2 and suPAR had the best prognostic performance (AUC = 0.7 [0.65-0.75]) compared to clinical or biological variables.
Conclusions: sVEGFR2, either alone or combined with suPAR, seems of interest to predict deterioration of patients with suspected bacterial acute infection upon ED admission and could help front-line physicians in the triage process.
Keywords: Biomarkers; Clinical deterioration; Emergency medicine; Endothelium; Prognosis; Sepsis.
Conflict of interest statement
MA Cazalis, S Blein and A Pachot are employees of bioMerieux SA. The other authors declare that they do not have any conflict of interest.
Figures

References
-
- Cecconi M, Evans L, Levy M, Rhodes A. Sepsis and septic shock. Lancet Lond Engl. 2018;392:75–87. - PubMed
LinkOut - more resources
Full Text Sources
