

The Effect of Advances in Lung-Cancer Treatment on Population Mortality
- PMID: 32786189
- PMCID: PMC8577315
- DOI: 10.1056/NEJMoa1916623
The Effect of Advances in Lung-Cancer Treatment on Population Mortality
Abstract
Background: Lung cancer is made up of distinct subtypes, including non-small-cell lung cancer (NSCLC) and small-cell lung cancer (SCLC). Although overall mortality from lung cancer has been declining in the United States, little is known about mortality trends according to cancer subtype at the population level because death certificates do not record subtype information.
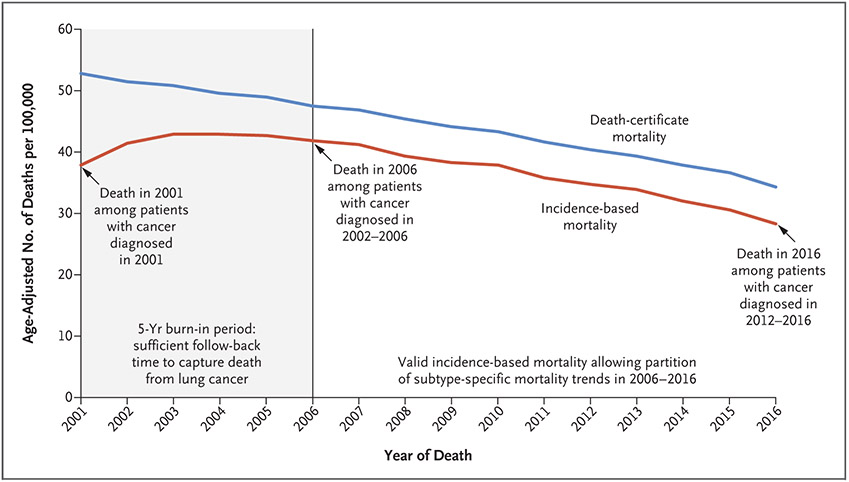
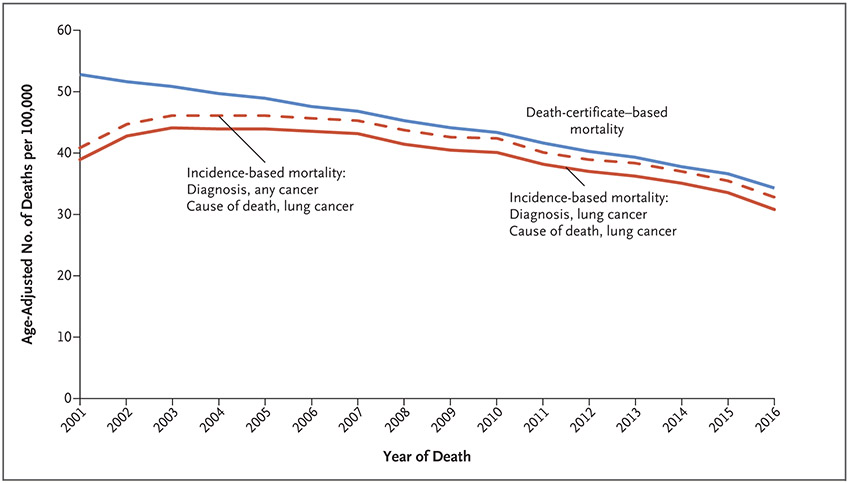
Methods: Using data from Surveillance, Epidemiology, and End Results (SEER) areas, we assessed lung-cancer mortality and linked deaths from lung cancer to incident cases in SEER cancer registries. This allowed us to evaluate population-level mortality trends attributed to specific subtypes (incidence-based mortality). We also evaluated lung-cancer incidence and survival according to cancer subtype, sex, and calendar year. Joinpoint software was used to assess changes in incidence and trends in incidence-based mortality.
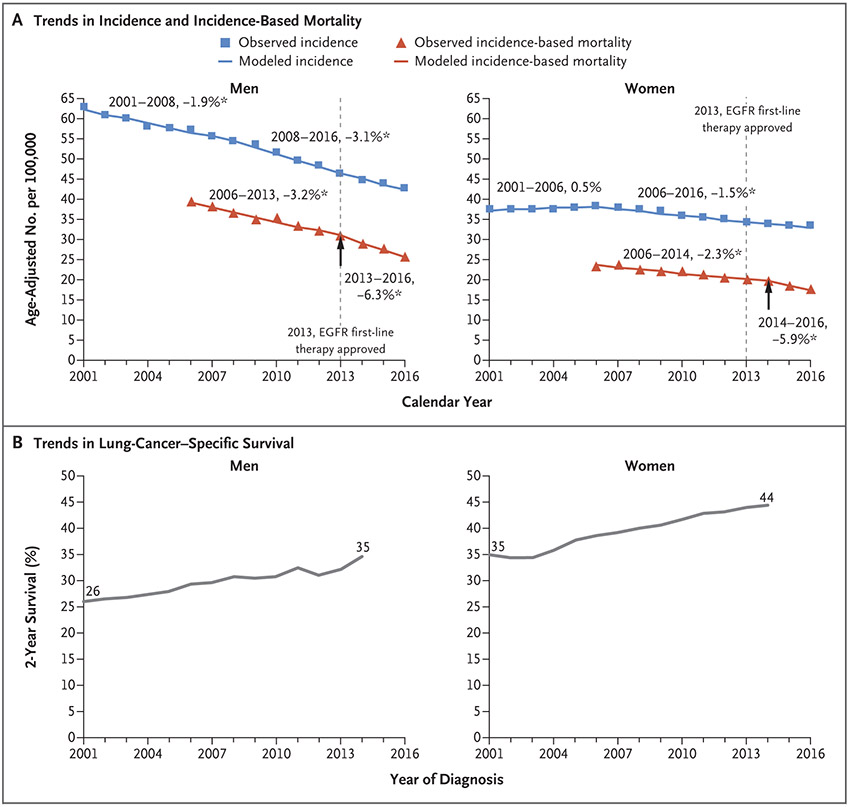
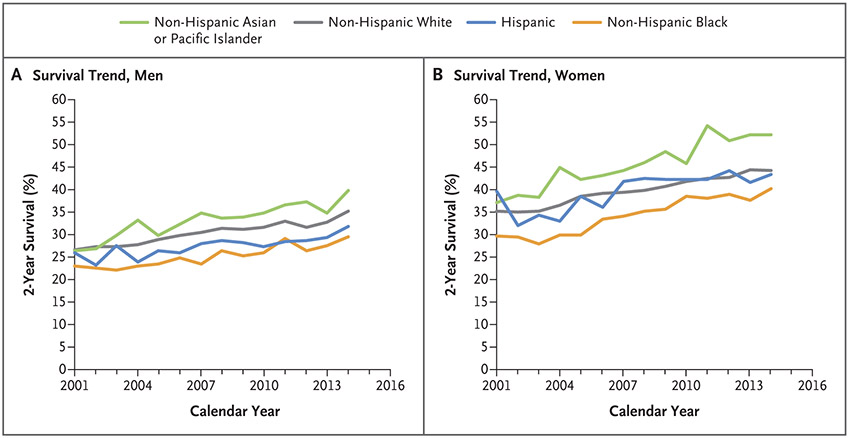
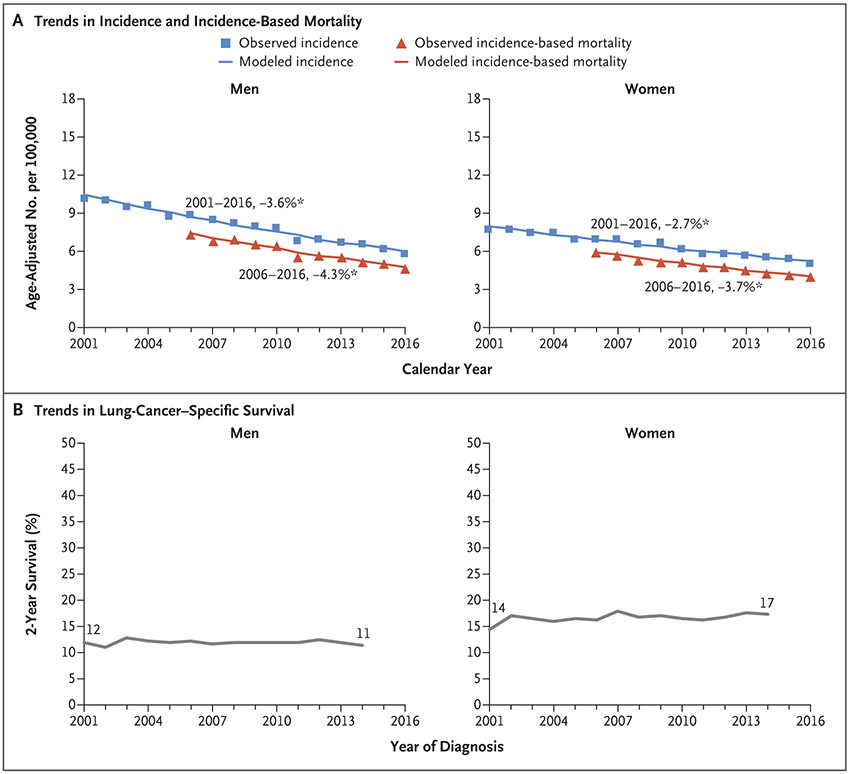
Results: Mortality from NSCLC decreased even faster than the incidence of this subtype, and this decrease was associated with a substantial improvement in survival over time that corresponded to the timing of approval of targeted therapy. Among men, incidence-based mortality from NSCLC decreased 6.3% annually from 2013 through 2016, whereas the incidence decreased 3.1% annually from 2008 through 2016. Corresponding lung cancer-specific survival improved from 26% among men with NSCLC that was diagnosed in 2001 to 35% among those in whom it was diagnosed in 2014. This improvement in survival was found across all races and ethnic groups. Similar patterns were found among women with NSCLC. In contrast, mortality from SCLC declined almost entirely as a result of declining incidence, with no improvement in survival. This result correlates with limited treatment advances for SCLC in the time frame we examined.
Conclusions: Population-level mortality from NSCLC in the United States fell sharply from 2013 to 2016, and survival after diagnosis improved substantially. Our analysis suggests that a reduction in incidence along with treatment advances - particularly approvals for and use of targeted therapies - is likely to explain the reduction in mortality observed during this period.
Copyright © 2020 Massachusetts Medical Society.
Figures
Comment in
-
Driving the Improvement of Lung Cancer Prognosis.Cancer Cell. 2020 Oct 12;38(4):449-451. doi: 10.1016/j.ccell.2020.09.008. Cancer Cell. 2020. PMID: 33049207
-
Immer weniger Lungenkrebs-Tote.MMW Fortschr Med. 2021 Jan;163(1):24. doi: 10.1007/s15006-021-9555-x. MMW Fortschr Med. 2021. PMID: 33464496 German. No abstract available.
-
Effect of stage shift and immunotherapy treatment on lung cancer survival outcomes.Eur J Cardiothorac Surg. 2023 Aug 1;64(2):ezad203. doi: 10.1093/ejcts/ezad203. Eur J Cardiothorac Surg. 2023. PMID: 37285318 Free PMC article.
References
-
- Travis WD, Brambilla E, Burke AP, Marx A, Nicholson AG. Introduction to the 2015 World Health Organization classification of tumors of the lung, pleura, thymus, and heart. J Thorac Oncol 2015;10:1240–2. - PubMed
-
- Howlader N, Krapcho M, Miller D, et al. SEER cancer statistics review, 1975-2016 [November 2018 SEER data submission posted to the SEER web site, April 9, 2020]. Bethesda, MD: National Cancer Institute; (https://seer.cancer.gov/csr/1975_2016/).
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical