

Multidrug resistant and extensively drug resistant Acinetobacter baumannii hospital infection associated with high mortality: a retrospective study in the pediatric intensive care unit
- PMID: 32787942
- PMCID: PMC7422664
- DOI: 10.1186/s12879-020-05321-y
Multidrug resistant and extensively drug resistant Acinetobacter baumannii hospital infection associated with high mortality: a retrospective study in the pediatric intensive care unit
Abstract
Background: Multidrug resistant (MDR) and extensively drug resistant (XDR) Acinetobacter baumannii presents challenges for clinical treatment and causes high mortality in children. We aimed to assess the risk factors and overall mortality for MDR/XDR Acinetobacter baumannii infected pediatric patients.
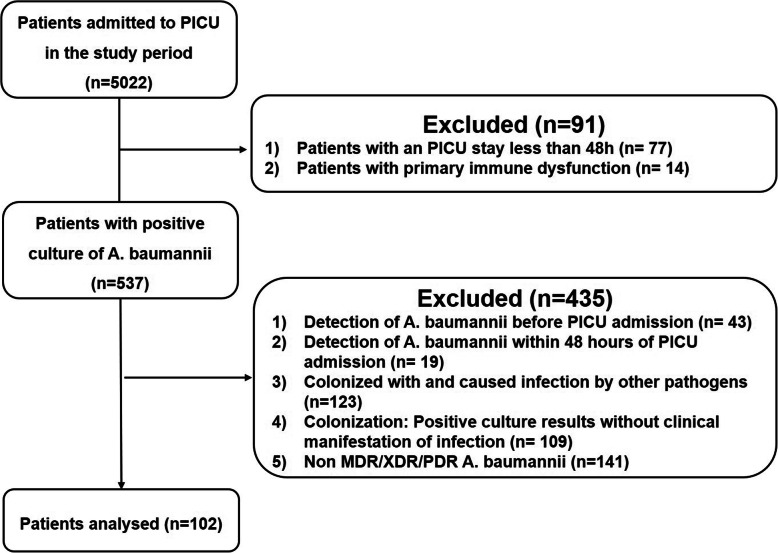
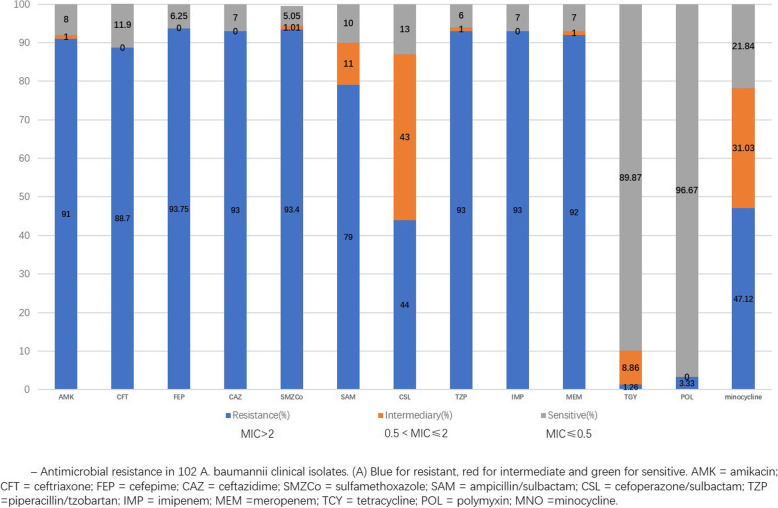
Methods: This retrospective study included 102 pediatric patients who developed MDR/XDR Acinetobacter baumannii infection in the pediatric intensive care unit (PICU) of Shanghai Children's Hospital in China from December 2014 to May 2018. Acinetobacter baumannii clinical isolates were recovered from different specimens including blood, sputum, bronchoalveolar lavage fluid, cerebrospinal fluid, ascites, hydrothorax, and urine. Antibiotic susceptibility test was determined according to the Clinical and Laboratory Standards Institute interpretive criteria. Clinical and biological data were obtained from the patients' medical records.
Results: 102 patients with Acinetobacter baumannii infection were enrolled. The median age was 36 (9.6, 98.8) months, and there were 63 male in the case group. The overall mortality rate was 29.4%, while the Acinetobacter baumannii-associated mortality rate was 16.7% (17/102, 12 bloodstream infections, 4 meningitis and 1 intra-abdominal infection). Bloodstream infections occurred in 28 patients (27.5%), and 10 patients (9.8%) among them had central line-associated bloodstream infections (6 central venous catheters, 2 PICCs, 1 venous infusion port and 1 arterial catheter). Cerebrospinal fluid (CSF) cultures were positive in 4(3.9%) patients. 14(13.7%) patients got positive cultures in ascites and hydrothorax. Lower respiratory isolates (56/102) accounted for 54.9% of all patients. Non-survival patients appeared to have a lower NK cell activity (6.2% ± 3.61% vs. 9.15% ± 6.21%, P = 0.029), higher CD4+ T cell ratio (39.67% ± 12.18% vs. 32.66% ± 11.44%, P = 0.039),and a higher serum level of interlukin-8 (IL-8, 15.25 (1.62, 47.22)pg/mL vs. 0.1 (0.1, 22.99)pg/mL, P = 0.01) when Acinetobacter baumannii infection developed. Multivariate logistic analysis indicated that high serum level of Cr (RR, 0.934, 95%CI, 0.890-0.981; P = 0.007) and high BUN/ALB level (RR, 107.893, 95%CI, 1.425-870.574; p = 0.005) were associated with high risk of mortality in MDR/XDR Acinetobacter baumannii infected patients.
Conclusion: MDR/XDR Acinetobacter baumannii infection is a serious concern in pediatric patients with high mortality. Bloodstream and central nervous system infection accounted for high risk of death. Acute kidney injury is associated with high risk of mortality.
Keywords: MDR/XDR, Acinetobacter baumannii; Mortality; Pediatric intensive care units; Risk factors.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Kempf M, Rolain JM. Emergence of resistance to carbapenems in Acinetobacter baumannii in Europe: clinical impact and therapeutic options. Int J Antimicrob Agents. 2012;39(2):105–114. - PubMed
-
- Nutman A, Glick R, Temkin E, et al. A case-control study to identify predictors of 14-day mortality following carbapenem-resistant Acinetobacter baumannii bacteraemia. Clin Microbiol Infect. 2014;20(12):O1028–O1034. - PubMed
-
- Karlowsky JA, Hoban DJ, Hackel MA, et al. Antimicrobial susceptibility of gram-negative ESKAPE pathogens isolated from hospitalized patients with intra-ABdominal and urinary tract infections in Asia-Pacific countries: SMART 2013-2015. J Med Microbiol. 2017;66(1):61–69. - PubMed
-
- Hackel MA, Badal RE, Bouchillon SK, et al. Resistance rates of intra-ABdominal isolates from intensive care units and non-intensive care units in the United States: the study for monitoring antimicrobial resistance trends 2010-2012. Surg Infect. 2015;16(3):298–304. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
