

Functional cognitive disorder: dementia's blind spot
- PMID: 32791521
- PMCID: PMC7586080
- DOI: 10.1093/brain/awaa224
Functional cognitive disorder: dementia's blind spot
Abstract
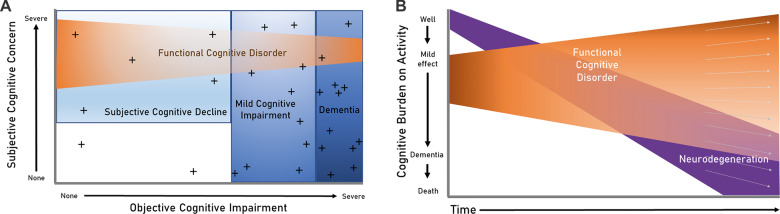
An increasing proportion of cognitive difficulties are recognized to have a functional cause, the chief clinical indicator of which is internal inconsistency. When these symptoms are impairing or distressing, and not better explained by other disorders, this can be conceptualized as a cognitive variant of functional neurological disorder, termed functional cognitive disorder (FCD). FCD is likely very common in clinical practice but may be under-diagnosed. Clinicians in many settings make liberal use of the descriptive term mild cognitive impairment (MCI) for those with cognitive difficulties not impairing enough to qualify as dementia. However, MCI is an aetiology-neutral description, which therefore includes patients with a wide range of underlying causes. Consequently, a proportion of MCI cases are due to non-neurodegenerative processes, including FCD. Indeed, significant numbers of patients diagnosed with MCI do not 'convert' to dementia. The lack of diagnostic specificity for MCI 'non-progressors' is a weakness inherent in framing MCI primarily within a deterministic neurodegenerative pathway. It is recognized that depression, anxiety and behavioural changes can represent a prodrome to neurodegeneration; empirical data are required to explore whether the same might hold for subsets of individuals with FCD. Clinicians and researchers can improve study efficacy and patient outcomes by viewing MCI as a descriptive term with a wide differential diagnosis, including potentially reversible components such as FCD. We present a preliminary definition of functional neurological disorder-cognitive subtype, explain its position in relation to other cognitive diagnoses and emerging biomarkers, highlight clinical features that can lead to positive diagnosis (as opposed to a diagnosis of exclusion), and red flags that should prompt consideration of alternative diagnoses. In the research setting, positive identifiers of FCD will enhance our recognition of individuals who are not in a neurodegenerative prodrome, while greater use of this diagnosis in clinical practice will facilitate personalized interventions.
Keywords: cognition; dementia; functional cognitive disorder; functional neurological disorder; mild cognitive impairment.
© The Author(s) (2020). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Functional cognitive disorder: dementia's blind spot.Brain. 2021 May 7;144(4):e37. doi: 10.1093/brain/awab008. Brain. 2021. PMID: 33837403 No abstract available.
References
-
- Albert MS, DeKosky ST, Dickson D, Dubois B, Feldman HH, Fox NC, et al.The diagnosis of mild cognitive impairment due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement 2011; 7: 270–9. - PMC - PubMed
-
- Alexander M, Blackburn D, Reuber M.. Patients' accounts of memory lapses in interactions between neurologists and patients with functional memory disorders. Sociol Health Illn 2019; 41: 249–65. - PubMed
-
- American Psychiatric Association. Somatic Symptom and Related Disorders. Diagnostic and statistical manual of mental disorders (DSM-5). 5th edn Washington, DC: American Psychiatric Publishing; 2013.
-
- Bailey C, Bell SM, Blackburn DM.. How the UK describes functional memory symptoms. Psychogeriatrics 2017; 17: 336–7. - PubMed
