

Correlations between clinical features and MRI findings in early adhesive capsulitis of the shoulder: a retrospective observational study
- PMID: 32791997
- PMCID: PMC7427071
- DOI: 10.1186/s12891-020-03569-8
Correlations between clinical features and MRI findings in early adhesive capsulitis of the shoulder: a retrospective observational study
Abstract
Background: This retrospective study investigated the association between clinical features and MRI findings in patients with early adhesive capsulitis of the shoulder.
Methods: The study included 29 patients with early adhesive capsulitis of the shoulder. The clinical diagnostic criteria were significantly restricted passive range of motion (ROM) and a symptom duration of up to 9 months. Various measurements related to adhesive capsulitis, including humeral and glenoid capsular thickness in the axillary recess, maximal axillary capsular thickness, coracohumeral ligament thickness, and anterior capsular thickness were measured on MRI. Abnormal humeral and glenoid capsular hyperintensity in the axillary recess, abnormal hyperintensity in the rotator interval, and obliteration of the subcoracoid fat triangle were also evaluated. Correlations between MRI findings and clinical features, including limited ROM, pain, and symptom duration were sought.
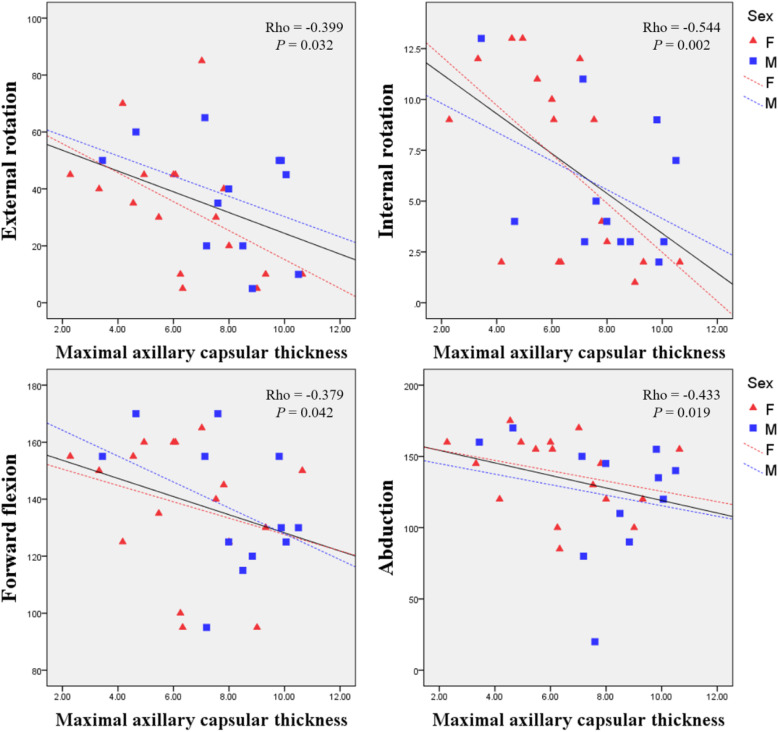
Results: Maximal axillary and humeral capsular thickness measured on MRI were negatively correlated with ROM for internal rotation. Also, hyperintensity in axillary recess and glenoid capule were correlated with ROM for abduction. Humeral capsular hyperintensity was correlated with ROM for forward flexion. There were no MRI findings that showed correlations with ROM for external rotation and severity of pain. The hyperintensity in the humeral capsule among MRI findings was only correlated with duration of symptoms.
Conclusions: MRI can be useful for assessment of several measures of clinical impairment in patients with adhesive capsulitis. Thickening and hyperintensity of the joint capsule in the axillary recess on MRI is associated with limited ROM and duration of symptoms.
Keywords: Adhesive capsulitis; Magnetic resonance imaging; Range of motion; Shoulder; pain.
Conflict of interest statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Figures

References
-
- Miller MD, Wirth MA, Rockwood CA. Thawing the frozen shoulder: the" patient" patient. Orthopedics. 1996;19:849–853. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
