

Prognostic impact of Borrmann classification on advanced gastric cancer: a retrospective cohort from a single institution in western China
- PMID: 32792016
- PMCID: PMC7427284
- DOI: 10.1186/s12957-020-01987-5
Prognostic impact of Borrmann classification on advanced gastric cancer: a retrospective cohort from a single institution in western China
Abstract
Background: Due to the controversy over the prognostic significance of Borrmann type in patients with gastric cancer (GC), the present study was to investigate the clinical value of Borrmann type in advanced GC.
Methods: We retrospectively evaluated 2092 patients with advanced GC and subsequently examined the clinicopathological characteristics and prognosis of patients stratified by Borrmann type.
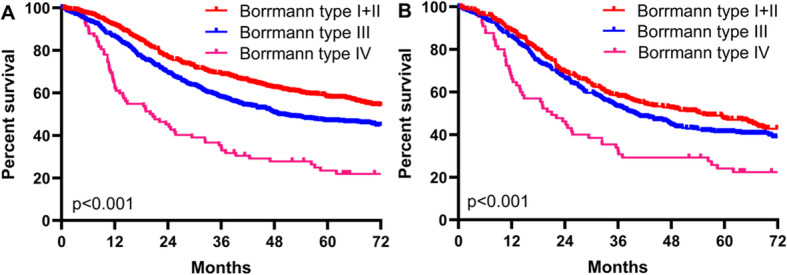
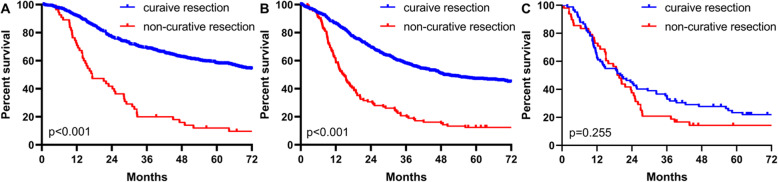
Results: Patients were divided into three groups according to Borrmann type (Borrmann types I+II, III, and IV). Patients with Borrmann types III and IV had larger size, more poorly differentiated tumor type, more advanced tumor stage, and higher chance of involving the entire stomach. The overall survival (OS) rates were significantly different among the three groups (p < 0.001). Stratification analysis revealed significant OS rates among the three groups in tumor-node-metastasis (TNM) stage III (p < 0.001) and TNM stage IV (p = 0.008). Multivariate analysis revealed that Borrmann types, adjuvant chemotherapy, curative resection, and TNM stage were all independent predictors of OS among GC patients. The subgroup analysis indicated that Borrmann type was an independent predictor of OS among GC patients who undergone curative resection and with TNM stage III cancer. However, curative resection and postoperative chemotherapy failed to prolong the survival of patients with Borrmann type IV.
Conclusions: The clinicopathological characteristics and prognosis of patients with three Borrmann types of GC were different. Borrmann type can be simply used as a valuable factor to predict survival in advanced GC patients, especially in those TNM stage III undergoing curative resection. Additionally, more attention should be paid to the treatment for Borrmann type IV GC.
Keywords: Borrmann type; Clinicopathological features; Gastric cancer; Prognosis.
Conflict of interest statement
The authors indicate no potential conflicts of interest.
Figures




References
-
- Macdonald JS, Smalley SR, Benedetti J, Hundahl SA, Estes NC, Stemmermann GN, Haller DG, Ajani JA, Gunderson LL, Jessup JM, et al. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N Engl J Med. 2001;345(10):725–730. doi: 10.1056/NEJMoa010187. - DOI - PubMed
-
- Yokota T, Ishiyama S, Saito T, Teshima S, Narushima Y, Murata K, Iwamoto K, Yashima R, Yamauchi H, Kikuchi S. Lymph node metastasis as a significant prognostic factor in gastric cancer: a multiple logistic regression analysis. Scand J Gastroenterol. 2004;39(4):380–384. doi: 10.1080/00365520310008629. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
