

Effect of liberal versus restrictive fluid therapy on intraoperative lactate levels in robot- assisted colorectal surgery
- PMID: 32792736
- PMCID: PMC7413354
- DOI: 10.4103/ija.IJA_401_20
Effect of liberal versus restrictive fluid therapy on intraoperative lactate levels in robot- assisted colorectal surgery
Abstract
Background and aims: Minimally invasive and robotic surgeries need lesser fluid replacement but the role of restricted fluids in robotic surgeries other than prostatic surgeries has not been clearly defined. Our primary aim was to evaluate the effects of a restrictive fluid regimen versus a liberal policy on intra-operative lactate in robotic colorectal surgery. Secondary outcomes were need for vasopressors, extubation on table, post-operative renal functions and length of ICU (LOICU) stay.
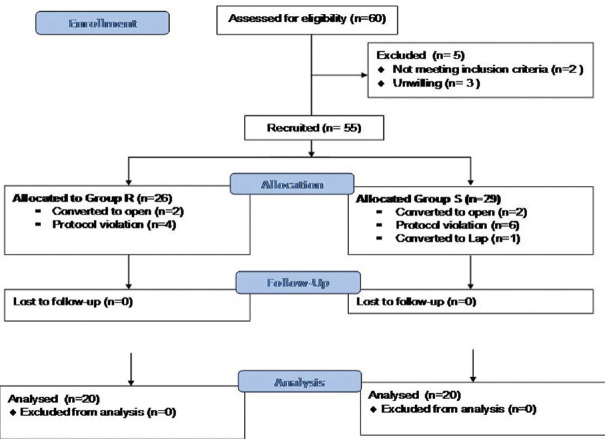
Methods: American society of anaesthesiologists (ASA) physical status I-II patients scheduled for robot-assisted colorectal surgery were randomised into one of two groups, receiving either 2 mL/kg/h (Group R) or 4mL/kg/h, (group L). Fluid boluses of 250 ml were administered if mean arterial pressure (MAP) <65 mmHg or urine output <0.5 ml/kg/h. Norepinephrine was added for the blood pressure after 2 fluid boluses. Surgical field was assessed by modified Boezaart's scale and surgeon satisfaction by Likert scale.
Results: Demographics and baseline renal functions were comparable. Adjusted intra-operative lactate at 2 h, 4 h, and 6 h and need for noradrenaline and post-operative creatinine were similar. One patient in the group L was ventilated due to hypothermia. The field was better at the 4 h in group R and comparable at other time points. The LOICU stay was longer in Group L.
Conclusion: The use of restrictive fluid strategy of 2 mL/kg/h (group R) does not increase lactate levels or creatinine, improves surgical field at 4 h and shortens ICU stay in comparison to a liberal 4 mL/kg/h (group L) in robotic colorectal surgery.
Keywords: Lactate; restrictive fluid therapy; robotic colorectal surgery.
Copyright: © 2020 Indian Journal of Anaesthesia.
Conflict of interest statement
There are no conflicts of interest.
Similar articles
-
Post-operative outcomes of intra-operative restrictive and conventional fluid management in laparoscopic colorectal cancer surgery.J Minim Access Surg. 2023 Apr-Jun;19(2):239-244. doi: 10.4103/jmas.jmas_19_22. J Minim Access Surg. 2023. PMID: 35915517 Free PMC article.
-
Does Restrictive Fluid Strategy during Robotic Pelvic Surgeries Obtund Intraoperative Rise in Intraocular Pressure?Anesth Essays Res. 2018 Jan-Mar;12(1):155-158. doi: 10.4103/aer.AER_144_17. Anesth Essays Res. 2018. PMID: 29628573 Free PMC article.
-
The Effect of Adding Dopamine Infusion to Noradrenaline Infusion Combined With Restrictive Hydration on Renal Function and Tissue Perfusion during Open Abdominal Surgeries.Anesth Essays Res. 2019 Apr-Jun;13(2):229-235. doi: 10.4103/aer.AER_34_19. Anesth Essays Res. 2019. PMID: 31198236 Free PMC article.
-
Robot-assisted surgery in elderly and very elderly population: our experience in oncologic and general surgery with literature review.Aging Clin Exp Res. 2017 Feb;29(Suppl 1):55-63. doi: 10.1007/s40520-016-0676-5. Epub 2016 Nov 30. Aging Clin Exp Res. 2017. PMID: 27905087 Review.
-
Perioperative liberal versus restrictive fluid strategies and postoperative outcomes: a systematic review and metanalysis on randomised-controlled trials in major abdominal elective surgery.Crit Care. 2021 Jun 11;25(1):205. doi: 10.1186/s13054-021-03629-y. Crit Care. 2021. PMID: 34116707 Free PMC article.
Cited by
-
Restricted Versus Liberal Versus Goal-Directed Fluid Therapy for Non-vascular Abdominal Surgery: A Network Meta-Analysis and Systematic Review.Cureus. 2023 Apr 28;15(4):e38238. doi: 10.7759/cureus.38238. eCollection 2023 Apr. Cureus. 2023. PMID: 37261162 Free PMC article. Review.
-
Comparison of arterial to end-tidal carbon dioxide gradient P (a-ET)CO2 in volume versus pressure controlled ventilation in patients undergoing robotic abdominal surgery in the Trendelenburg position. A randomised controlled study.Indian J Anaesth. 2022 Aug;66(Suppl 5):S243-S249. doi: 10.4103/ija.ija_902_21. Epub 2022 Aug 12. Indian J Anaesth. 2022. PMID: 36262723 Free PMC article.
-
Unilateral compartment syndrome of the lower limbs after robotic radical cystectomy and ileal conduit.Indian J Anaesth. 2022 Feb;66(2):160-162. doi: 10.4103/ija.ija_63_21. Epub 2022 Feb 24. Indian J Anaesth. 2022. PMID: 35359464 Free PMC article. No abstract available.
-
The ten essential "T's" imparting impetus to research in anaesthesiology.Indian J Anaesth. 2020 Jul;64(7):551-555. doi: 10.4103/ija.IJA_829_20. Epub 2020 Jul 1. Indian J Anaesth. 2020. PMID: 32792732 Free PMC article. No abstract available.
-
Biochemical implications of robotic surgery: a new frontier in the operating room.J Robot Surg. 2024 Feb 24;18(1):91. doi: 10.1007/s11701-024-01861-6. J Robot Surg. 2024. PMID: 38401027 Review.
References
-
- Irvine M, Patil V. Anaesthesia for robot-assisted laparoscopic surgery. CEACCP. 2009;4:125–79.
-
- Doherty M, Buggy DJ. Intraoperative fluids: How much is toomuch? Br J Anaesth. 2012;109:69–79. - PubMed
LinkOut - more resources
Full Text Sources