

Improving Function in Cavernous Sinus Meningiomas: A Modern Treatment Algorithm
- PMID: 32793095
- PMCID: PMC7393208
- DOI: 10.3389/fneur.2020.00652
Improving Function in Cavernous Sinus Meningiomas: A Modern Treatment Algorithm
Abstract
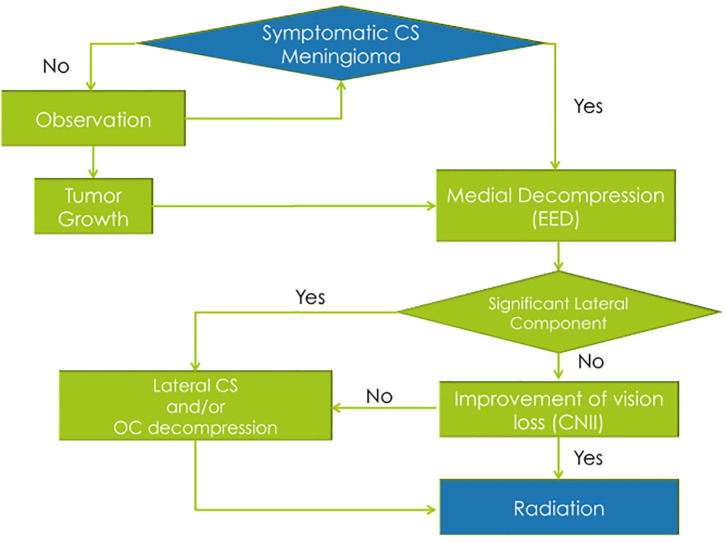
Background: The efficacy and safety of radiosurgery led to paradigm shift in the management of cavernous sinus meningiomas. Nevertheless, patients are still significantly affected by cranial nerve deficits related to the mass effect of these tumors. Our management strategy involves the combination of a functional surgical decompression followed by radiation therapy. Methods: We reviewed a single institution's cohort of patients who underwent endoscopic endonasal decompression (EED) for symptomatic meningiomas primarily involving the cavernous sinus (CS) from 2010 to 2016. The preoperative neuro-ophthalmological exam was compared to the 1- and 6-month postoperative exams. The patient's length of hospital stay, complications, and radiological and clinical follow-up were noted. Results: A total of 17 patients underwent EED for CS meningiomas that fit our radiological criteria. The final outcome at the 6-month visit showed five patients (62.5%) with normalization of deficit and three patients (37.5%) with partial improvement of the CNII deficit. Out of the 12 patients who had cavernous sinus cranial nerves (CSCN) deficits, the final outcome at the 6-month visit showed four patients (33.33%) with normalization of deficit, seven patients (58.3%) with partial improvement, and one patient (8.33%) with no improvement. There were no intraoperative complications. Conclusion: The EED for CS meningiomas is a valuable technique when addressing acute/subacute CNII and CSCN deficits. This conservative surgical approach showed good functional outcomes, low morbidity, and low complication rates. However, it does not exempt the need for radiosurgery/radiation therapy for control of tumor growth.
Keywords: cavernous sinus; endoscopic endonasal; meningioma; parasellar; skull base.
Copyright © 2020 Beer-Furlan, Priddy, Jamshidi, Shaikhouni, Prevedello, Ditzel Filho, Otto, Carrau and Prevedello.
Figures
References
LinkOut - more resources
Full Text Sources