

US Mortality Attributable to Congenital Heart Disease Across the Lifespan From 1999 Through 2017 Exposes Persistent Racial/Ethnic Disparities
- PMID: 32795094
- PMCID: PMC7508797
- DOI: 10.1161/CIRCULATIONAHA.120.046822
US Mortality Attributable to Congenital Heart Disease Across the Lifespan From 1999 Through 2017 Exposes Persistent Racial/Ethnic Disparities
Abstract
Background: Congenital heart disease (CHD) accounts for ≈40% of deaths in US children with birth defects. Previous US data from 1999 to 2006 demonstrated an overall decrease in CHD mortality. Our study aimed to assess current trends in US mortality related to CHD from infancy to adulthood over the past 19 years and determine differences by sex and race/ethnicity.
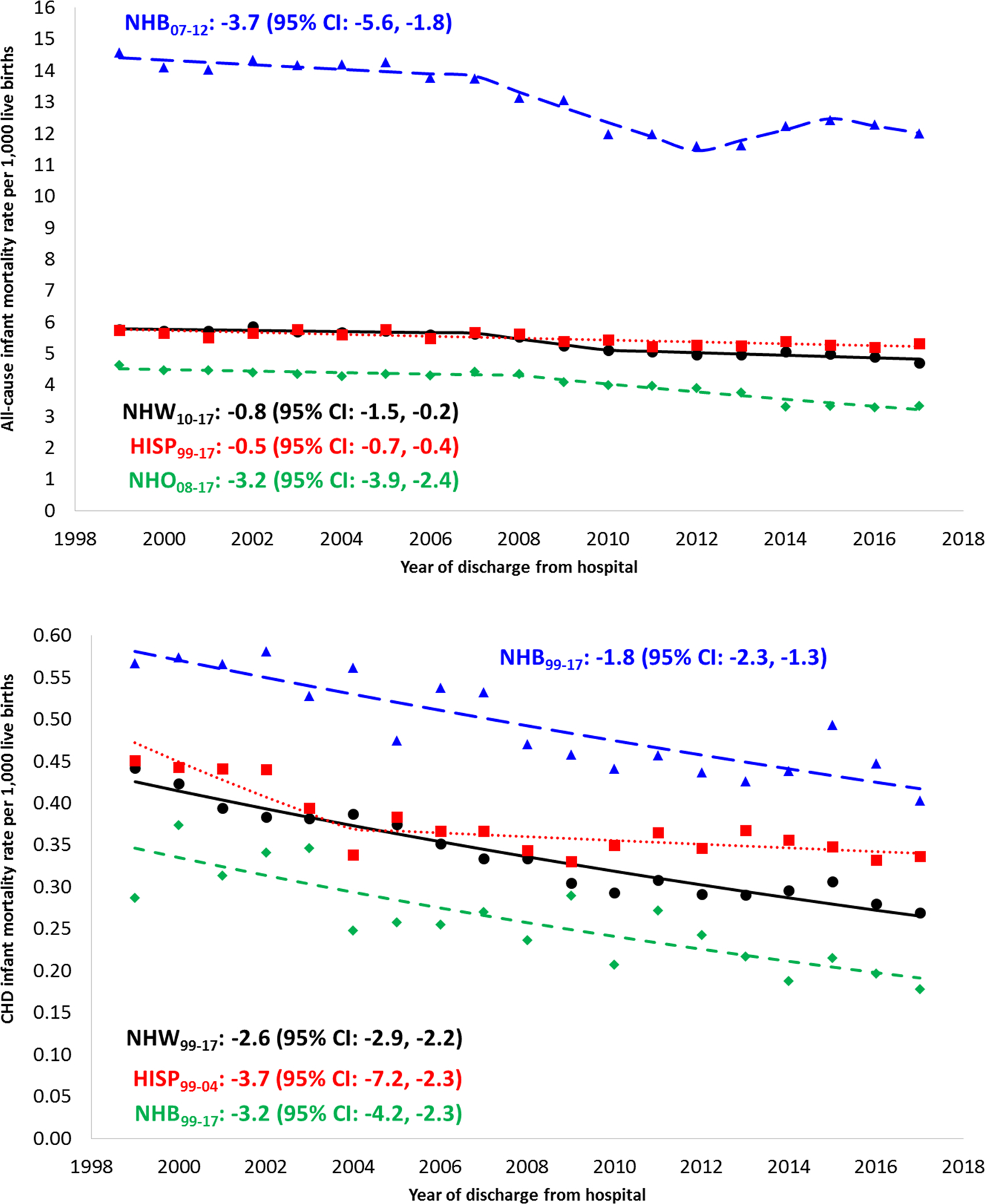
Methods: We conducted an analysis of death certificates from 1999 to 2017 to calculate annual CHD mortality by age at death, race/ethnicity, and sex. Population estimates used as denominators in mortality rate calculations for infants were based on National Center for Health Statistics live birth data. Mortality rates in individuals ≥1 year of age used US Census Bureau bridged-race population estimates as denominators. We used joinpoint regression to characterize temporal trends in all-cause mortality, mortality resulting directly attributable to and related to CHD by age, race/ethnicity, and sex.
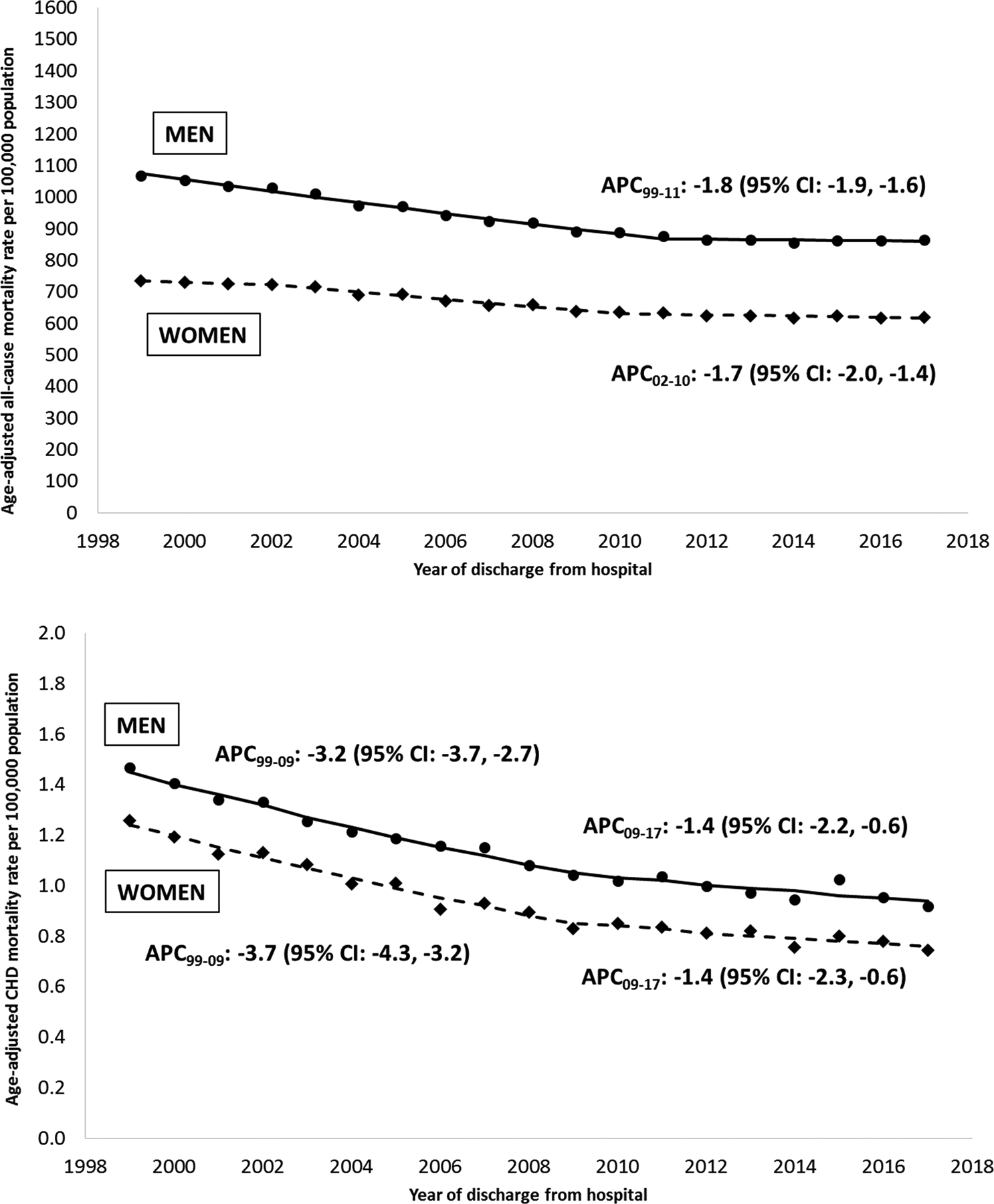
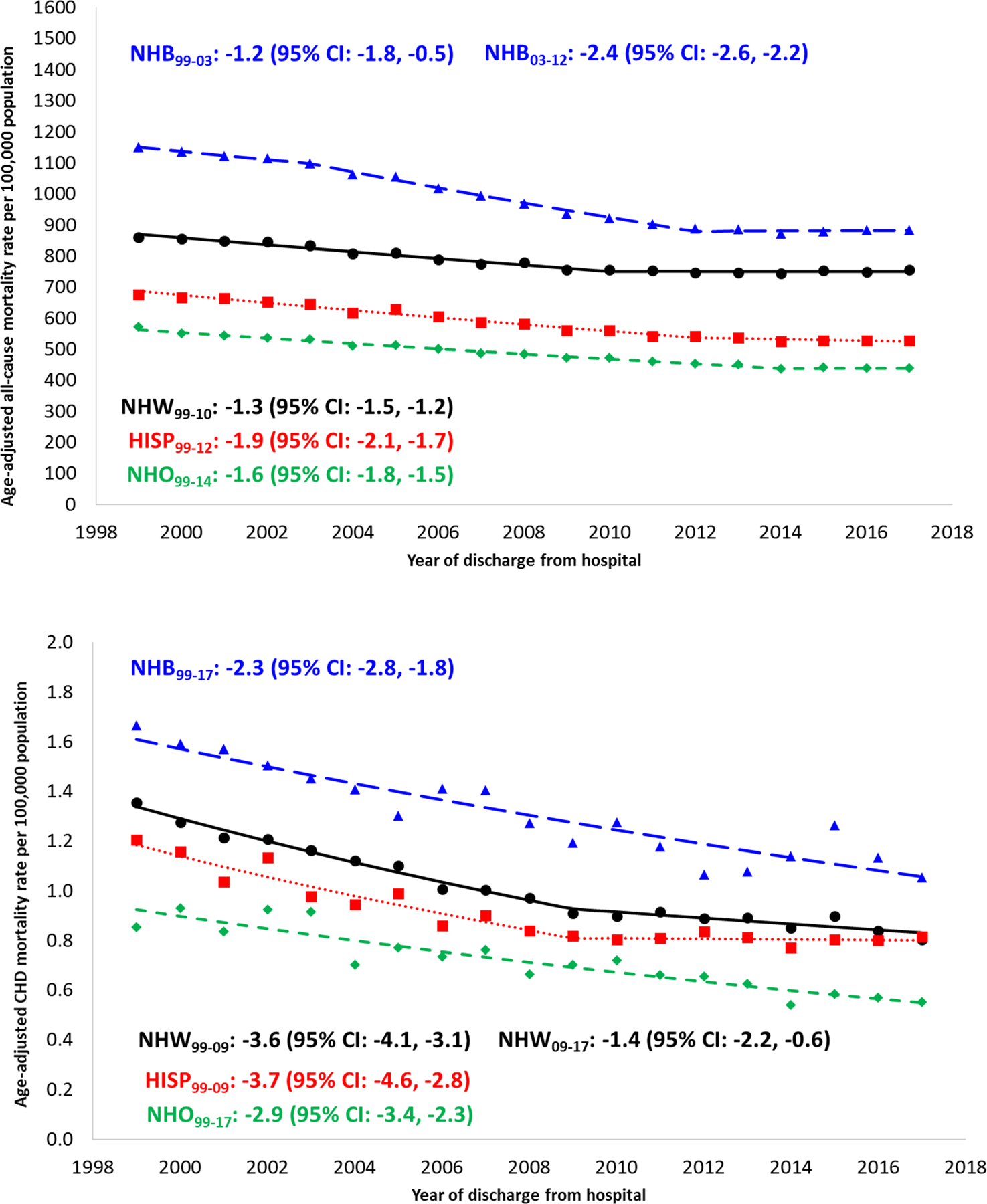
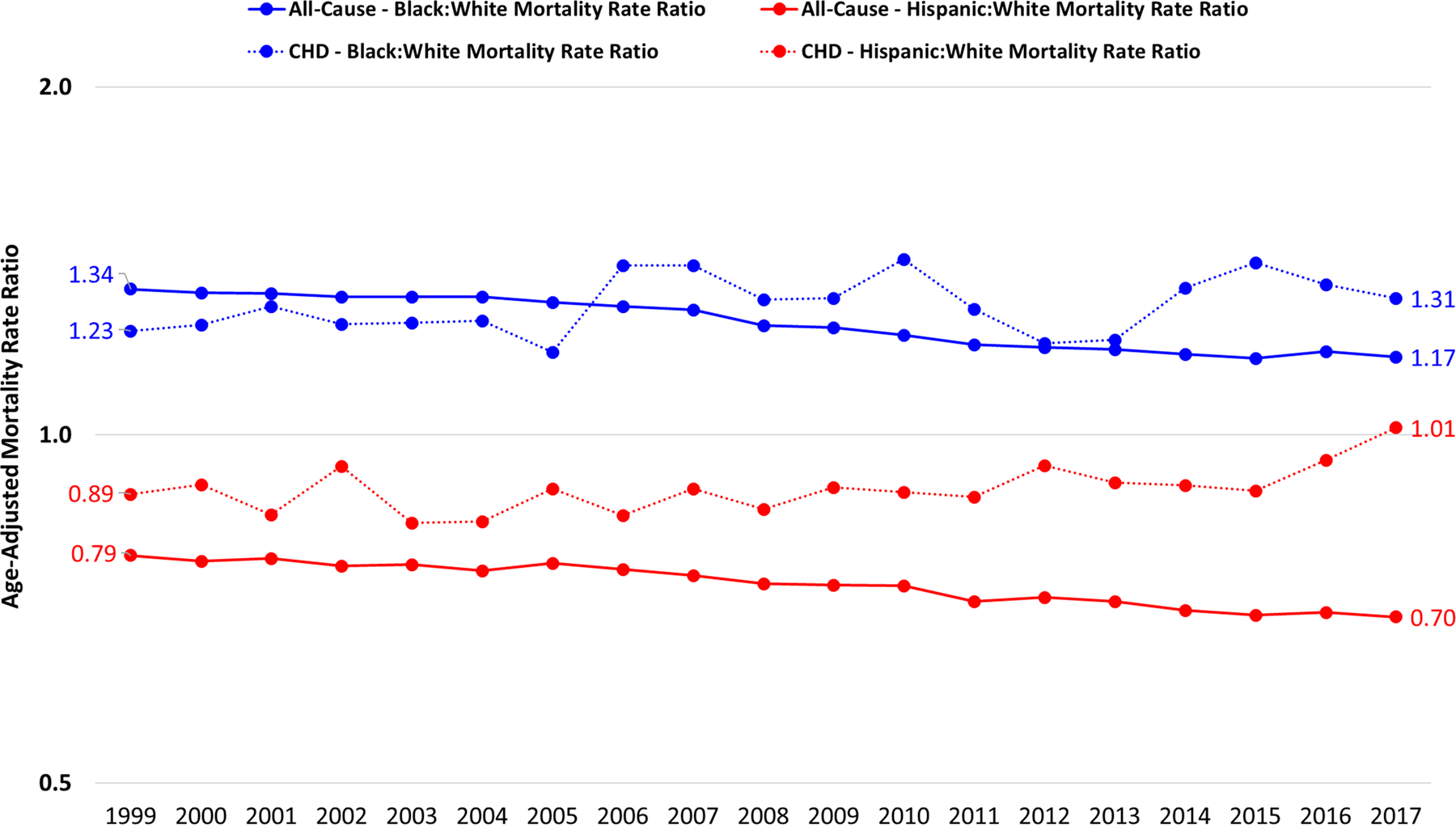
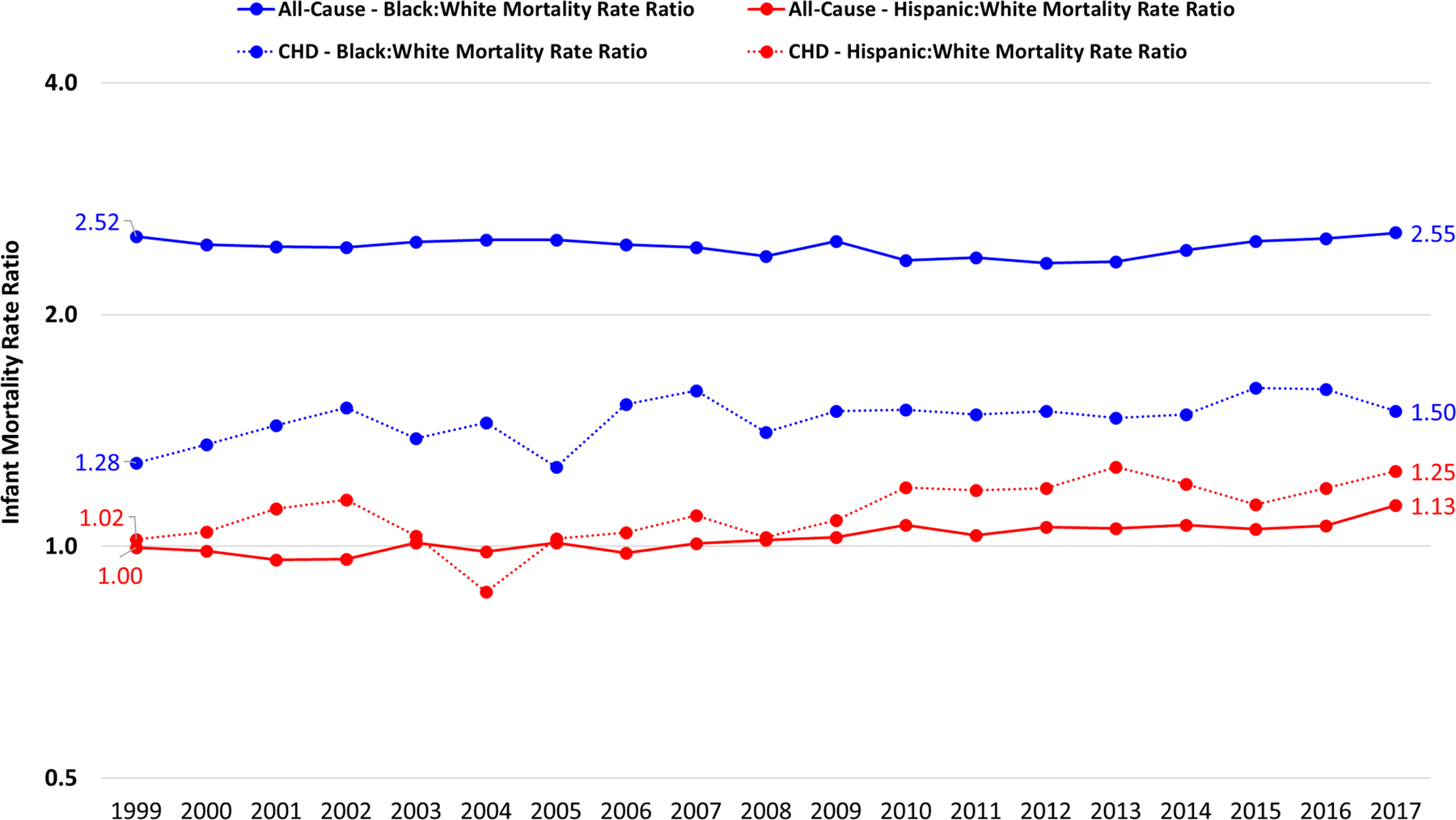
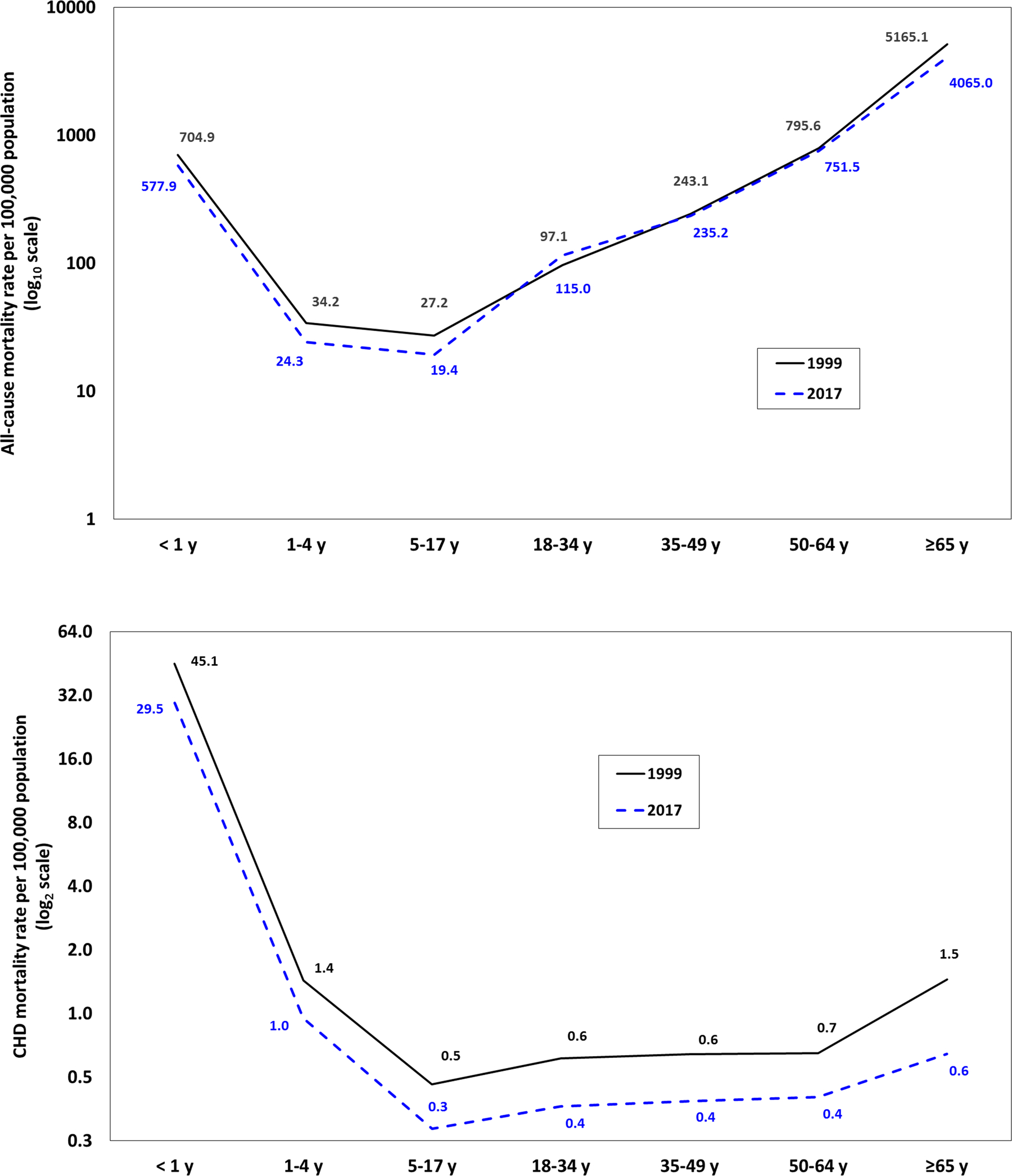
Results: There were 47.7 million deaths with 1 in 814 deaths attributable to CHD (n=58 599). Although all-cause mortality decreased 16.4% across all ages, mortality resulting from CHD declined 39.4% overall. The mean annual decrease in CHD mortality was 2.6%, with the largest decrease for those >65 years of age. The age-adjusted mortality rate decreased from 1.37 to 0.83 per 100 000. Males had higher mortality attributable to CHD than females throughout the study, although both sexes declined at a similar rate (≈40% overall), with a 3% to 4% annual decrease between 1999 and 2009, followed by a slower annual decrease of 1.4% through 2017. Mortality resulting from CHD significantly declined among all races/ethnicities studied, although disparities in mortality persisted for non-Hispanic Blacks versus non-Hispanic Whites (mean annual decrease 2.3% versus 2.6%, respectively; age-adjusted mortality rate 1.67 to 1.05 versus 1.35 to 0.80 per 100 000, respectively).
Conclusions: Although overall US mortality attributable to CHD has decreased over the past 19 years, disparities in mortality persist for males in comparison with females and for non-Hispanic Blacks in comparison with non-Hispanic Whites. Determining factors that contribute to these disparities such as access to quality care, timely diagnosis, and maintenance of insurance will be important moving into the next decade.
Keywords: healthcare disparities; heart diseases; longevity; mortality.
Conflict of interest statement
DISCLOSURES
The authors have no financial relationships relevant to this article to disclose.
Figures
References
-
- Yang Q, Khoury MJ, Mannino D. Trends and patterns of mortality associated with birth defects and genetic diseases in the United States, 1979–1992: An analysis of multiple-cause mortality data. Genet Epidemiol. 1997;14:493–505. - PubMed
-
- Petrini J, Damus K, Johnston RB. An overview of infant mortality and birth defects in the United States. Teratology. 1997;56:8–10. - PubMed
-
- Roncancio CP, Misnaza SP, Peña IC, Prieto FE, Cannon MJ, Valencia D. Trends and characteristics of fetal and neonatal mortality due to congenital anomalies, Colombia 1999–2008. J Maternal-fetal Neonatal Medicine Official J European Assoc Périnat Medicine Fed Asia Ocean Périnat Soc Int Soc Périnat Obstetricians. 2017;31:1748–1755. - PMC - PubMed
-
- World Health Organization. Global Health Estimates 2016: Disease Burden by Cause, Age, Sex, by Country and by Region 2000–2016. https://www.who.int/healthinfo/global_burden_disease/GlobalDALY_method_2... Published, Geneva, 2018. Accessed May 15, 2019.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
