

Rucaparib in Men With Metastatic Castration-Resistant Prostate Cancer Harboring a BRCA1 or BRCA2 Gene Alteration
- PMID: 32795228
- PMCID: PMC7655021
- DOI: 10.1200/JCO.20.01035
Rucaparib in Men With Metastatic Castration-Resistant Prostate Cancer Harboring a BRCA1 or BRCA2 Gene Alteration
Abstract
Purpose: BRCA1 or BRCA2 (BRCA) alterations are common in men with metastatic castration-resistant prostate cancer (mCRPC) and may confer sensitivity to poly(ADP-ribose) polymerase inhibitors. We present results from patients with mCRPC associated with a BRCA alteration treated with rucaparib 600 mg twice daily in the phase II TRITON2 study.
Methods: We enrolled patients who progressed after one to two lines of next-generation androgen receptor-directed therapy and one taxane-based chemotherapy for mCRPC. Efficacy and safety populations included patients with a deleterious BRCA alteration who received ≥ 1 dose of rucaparib. Key efficacy end points were objective response rate (ORR; per RECIST/Prostate Cancer Clinical Trials Working Group 3 in patients with measurable disease as assessed by blinded, independent radiology review and by investigators) and locally assessed prostate-specific antigen (PSA) response (≥ 50% decrease from baseline) rate.
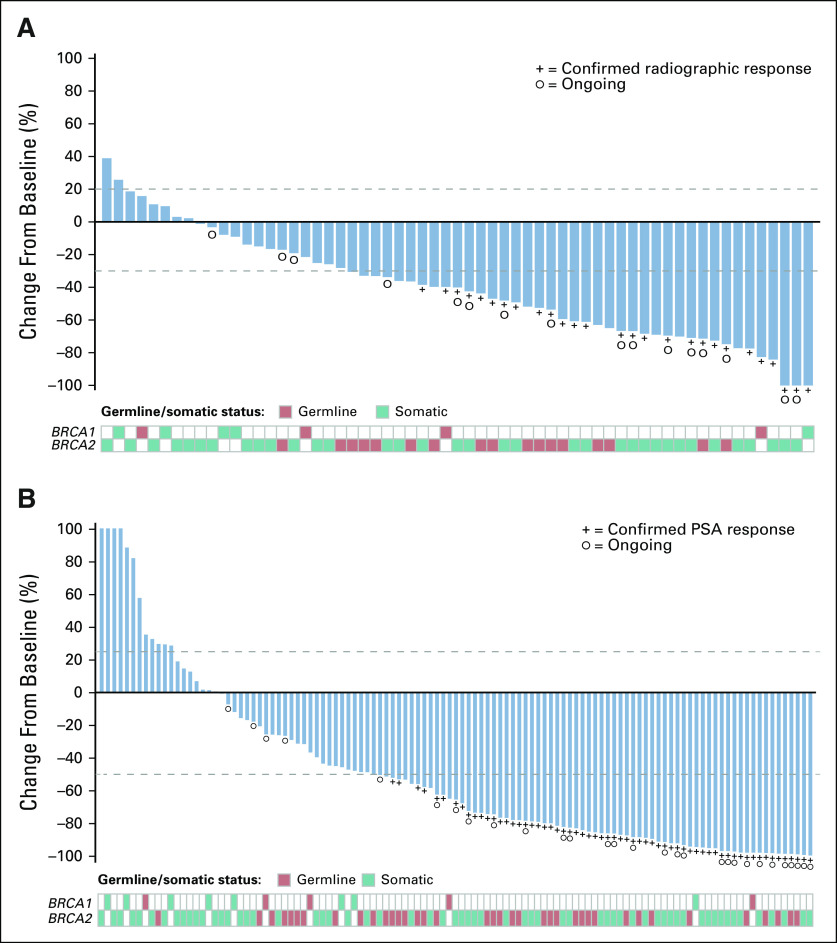
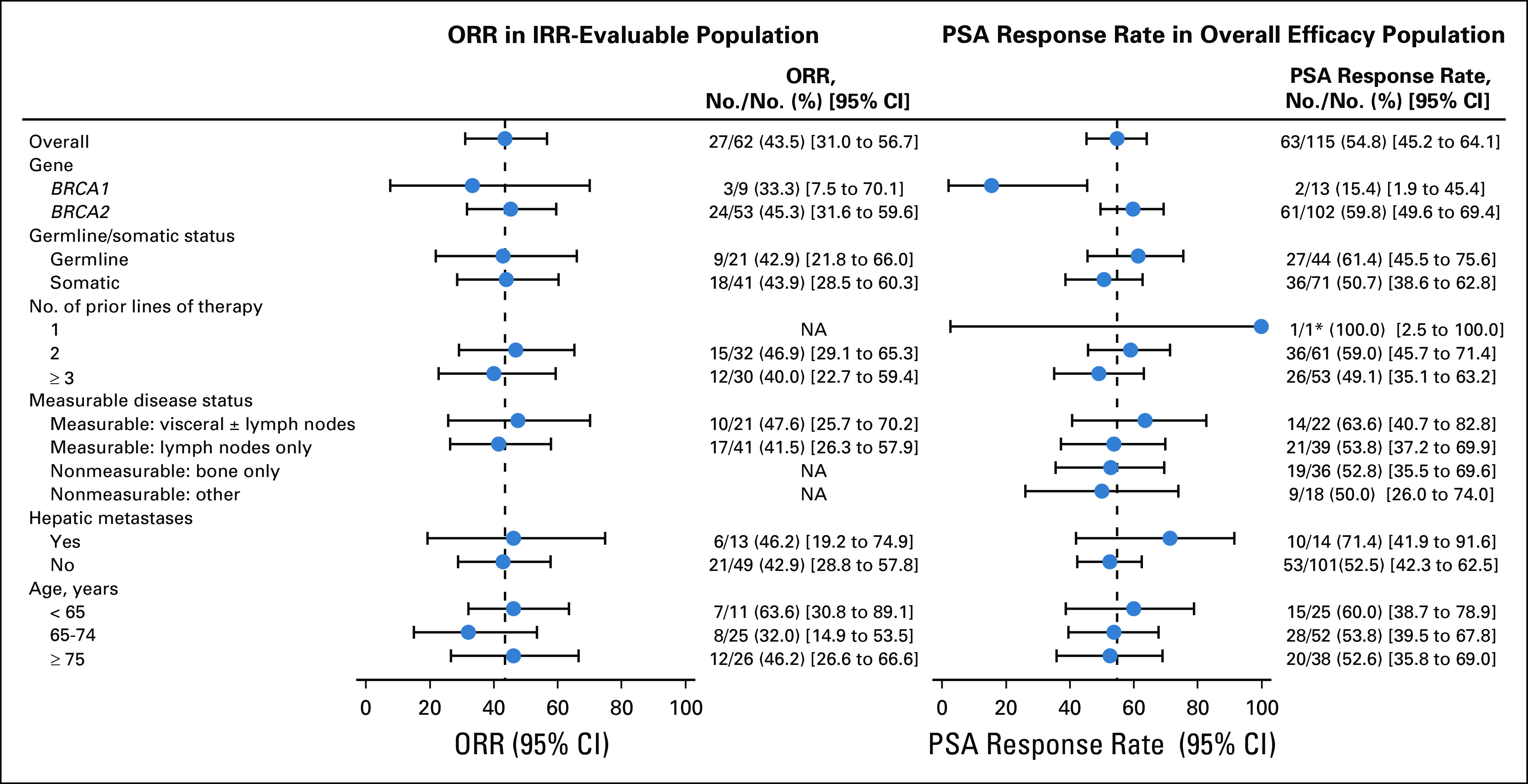
Results: Efficacy and safety populations included 115 patients with a BRCA alteration with or without measurable disease. Confirmed ORRs per independent radiology review and investigator assessment were 43.5% (95% CI, 31.0% to 56.7%; 27 of 62 patients) and 50.8% (95% CI, 38.1% to 63.4%; 33 of 65 patients), respectively. The confirmed PSA response rate was 54.8% (95% CI, 45.2% to 64.1%; 63 of 115 patients). ORRs were similar for patients with a germline or somatic BRCA alteration and for patients with a BRCA1 or BRCA2 alteration, while a higher PSA response rate was observed in patients with a BRCA2 alteration. The most frequent grade ≥ 3 treatment-emergent adverse event was anemia (25.2%; 29 of 115 patients).
Conclusion: Rucaparib has antitumor activity in patients with mCRPC and a deleterious BRCA alteration, but with a manageable safety profile consistent with that reported in other solid tumor types.
Figures
Comment in
-
BRCA1 Versus BRCA2 and PARP Inhibitor Sensitivity in Prostate Cancer: More Different Than Alike?J Clin Oncol. 2020 Nov 10;38(32):3735-3739. doi: 10.1200/JCO.20.02246. Epub 2020 Sep 1. J Clin Oncol. 2020. PMID: 32870734 Free PMC article. No abstract available.
References
-
- National Comprehensive Cancer Network NCCN Clinical Practice Guidelines in Oncology: Prostate cancer (version 2.2020) https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf
-
- Parker C, Gillessen S, Heidenreich A, et al. Cancer of the prostate: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2015;26:v69–v77. - PubMed
-
- European Association of Urology Guidelines: Prostate cancer. http://uroweb.org/guideline/prostate-cancer/
-
- Gillessen S, Attard G, Beer TM, et al. Management of patients with advanced prostate cancer: Report of the Advanced Prostate Cancer Consensus Conference 2019. Eur Urol. 2020;77:508–547. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
