

Clinical and laboratory evaluation of SARS-CoV-2 lateral flow assays for use in a national COVID-19 seroprevalence survey
- PMID: 32796119
- PMCID: PMC7430184
- DOI: 10.1136/thoraxjnl-2020-215732
Clinical and laboratory evaluation of SARS-CoV-2 lateral flow assays for use in a national COVID-19 seroprevalence survey
Abstract
Background: Accurate antibody tests are essential to monitor the SARS-CoV-2 pandemic. Lateral flow immunoassays (LFIAs) can deliver testing at scale. However, reported performance varies, and sensitivity analyses have generally been conducted on serum from hospitalised patients. For use in community testing, evaluation of finger-prick self-tests, in non-hospitalised individuals, is required.
Methods: Sensitivity analysis was conducted on 276 non-hospitalised participants. All had tested positive for SARS-CoV-2 by reverse transcription PCR and were ≥21 days from symptom onset. In phase I, we evaluated five LFIAs in clinic (with finger prick) and laboratory (with blood and sera) in comparison to (1) PCR-confirmed infection and (2) presence of SARS-CoV-2 antibodies on two 'in-house' ELISAs. Specificity analysis was performed on 500 prepandemic sera. In phase II, six additional LFIAs were assessed with serum.
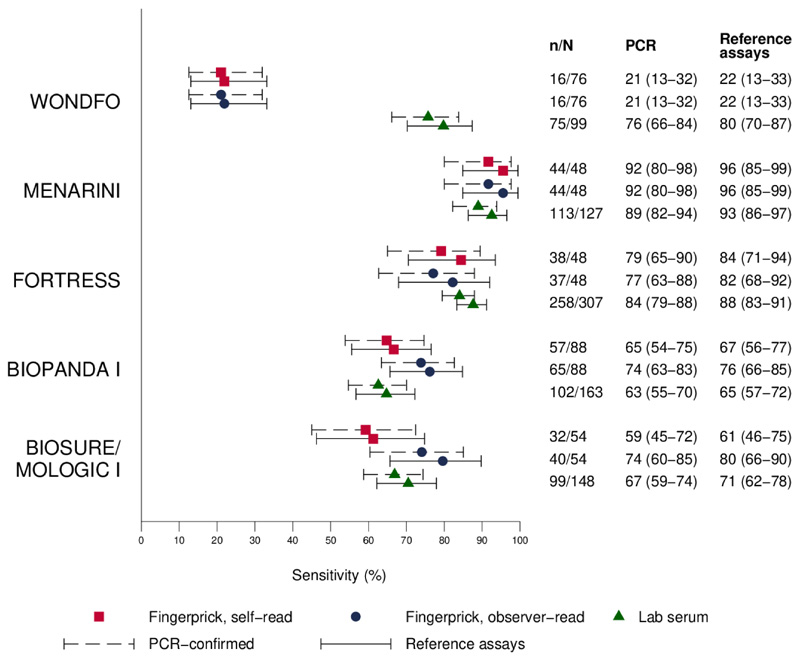
Findings: 95% (95% CI 92.2% to 97.3%) of the infected cohort had detectable antibodies on at least one ELISA. LFIA sensitivity was variable, but significantly inferior to ELISA in 8 out of 11 assessed. Of LFIAs assessed in both clinic and laboratory, finger-prick self-test sensitivity varied from 21% to 92% versus PCR-confirmed cases and from 22% to 96% versus composite ELISA positives. Concordance between finger-prick and serum testing was at best moderate (kappa 0.56) and, at worst, slight (kappa 0.13). All LFIAs had high specificity (97.2%-99.8%).
Interpretation: LFIA sensitivity and sample concordance is variable, highlighting the importance of evaluations in setting of intended use. This rigorous approach to LFIA evaluation identified a test with high specificity (98.6% (95%CI 97.1% to 99.4%)), moderate sensitivity (84.4% with finger prick (95% CI 70.5% to 93.5%)) and moderate concordance, suitable for seroprevalence surveys.
Keywords: clinical epidemiology; respiratory infection; viral infection.
© Author(s) (or their employer(s)) 2020. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- FIND. SARS-CoV-2 diagnostic pipeline. Published 2020. Available: https://www.fnddx.org/covid-19/pipeline/
-
- Department for Health and Social Care. Coronavirus (COVID-19) scaling up our testing programmes. Available: https://assets.publishing.service.gov.uk/government/uploads/system/uploa....
-
- Whitman JD, Hiatt J, Mowery CT, et al. Test performance evaluation of SARS-CoV-2 serological assays. medRxiv. 2020 2020042520074856.
-
- Lassaunière R, Frische A. Evaluation of nine commercial SARS-CoV-2 immunoassays. medRxiv
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous