

Short- and long-term outcome of patients with aneurysmal subarachnoid hemorrhage
- PMID: 32796129
- PMCID: PMC7682825
- DOI: 10.1212/WNL.0000000000010618
Short- and long-term outcome of patients with aneurysmal subarachnoid hemorrhage
Abstract
Objective: To describe short-term and 5-year rates of mortality and poor outcome in patients with spontaneous aneurysmal subarachnoid hemorrhage (aSAH) who received repair treatment.
Methods: In this prospective observational study, mortality and poor outcome (modified Rankin Scale score 3-6) were analyzed in 311 patients with aSAH at 3 months, 1 year, and 5 years follow-up. Sensitivity analysis was performed according to treatment modality. In-hospital and 5-year complications were analyzed.
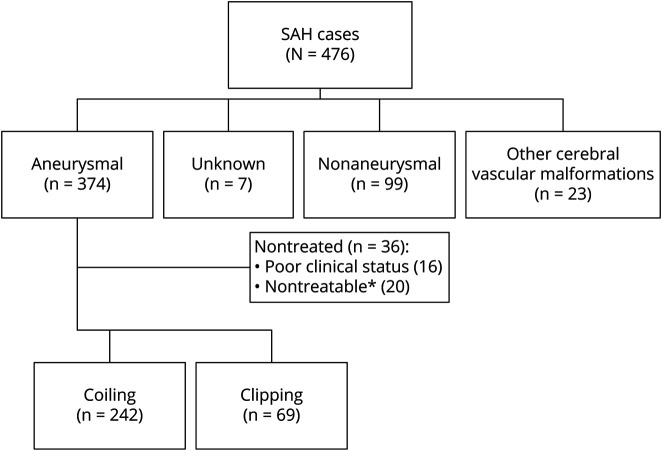
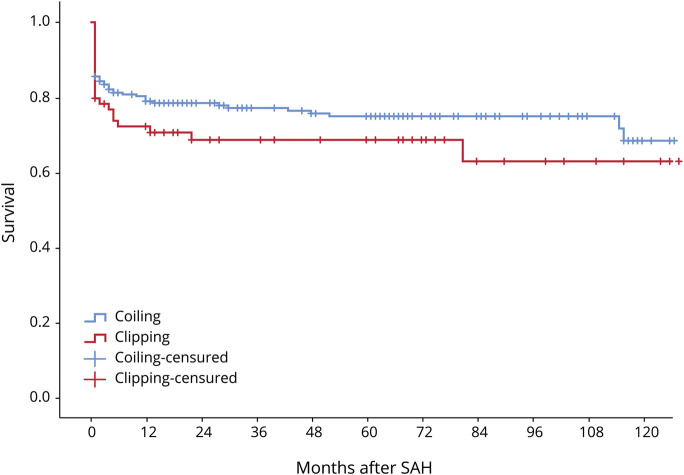
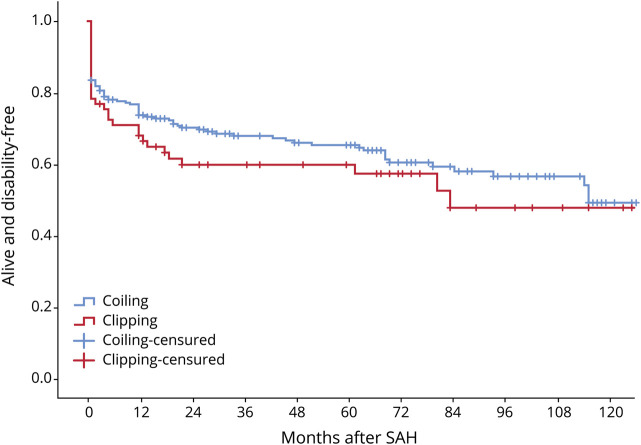
Results: Of 476 consecutive patients with spontaneous subarachnoid hemorrhage, 347 patients (72.9%) had aSAH. Of these, 311 (89.6%) were treated (242 endovascular, 69 neurosurgical), with a mean follow-up of 43.4 months (range, 1 to 145). Three-month, 1-year, and 5-year mortality was 18.4%, 22.9%, and 29.0%, and poor outcome was observed in 42.3%, 36.0%, and 36.0%, respectively. Adjusted poor outcome was lower in endovascular than in neurosurgical treatment at 3 months (odds ratio [OR] 0.36 [95% confidence interval [CI] 0.18-0.74]), with an absolute difference of 15.8% (number needed to treat = 6.3), and at 1 year (OR = 0.40 [95% CI 0.20-0.81]), with an absolute difference of 15.9% (number needed to treat = 6.3). Complications did not differ between the 2 procedures. However, mechanical ventilation was less frequent with the endovascular technique (OR 0.67 [95% CI 0.54-0.84]).
Conclusions: Patients with aSAH treated according to current guidelines had a short-term mortality of 18.4% and 5-year mortality of 29%. The majority (64.0%) of patients remained alive without disabilities at 5-year follow-up. Patients prioritized to endovascular treatment had better outcomes than those referred to neurosurgery because endovascular coiling was not feasible.
© 2020 American Academy of Neurology.
Figures
Comment in
- Neurology. 95(13):e1915. doi: 10.1212/WNL.0000000000010642
References
-
- MacDonald RL, Schweizer TA. Spontaneous subarachnoid hemorrhage. Lancet 2017;389:655–666. - PubMed
-
- Steiner T, Juvela S, Unterberg A, Jung C, Forsting M, Rinkel G. European Stroke Organization guidelines for the management of intracranial aneurysms and subarachnoid haemorrhage. Cerebrovasc Dis 2013;35:93–112. - PubMed
-
- Nieuwkamp DJ, Setz LE, Algra A, Linn FH, de Rooij NK, Rinkel GJ. Changes in case fatality of aneurysmal subarachnoid haemorrhage over time, according to age, sex, and region: a meta-analysis. Lancet Neurol 2009;8:635–642. - PubMed
-
- Vergouwen MD, Jong-Tjien-Fa AV, Algra A, Rinkel GJ. Time trends in causes of death after aneurysmal subarachnoid hemorrhage: a hospital-based study. Neurology 2016;86:59–63. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical