

Clinical Utility and Cost Savings in Predicting Inadequate Response to Anti-TNF Therapies in Rheumatoid Arthritis
- PMID: 32797404
- PMCID: PMC7695768
- DOI: 10.1007/s40744-020-00226-3
Clinical Utility and Cost Savings in Predicting Inadequate Response to Anti-TNF Therapies in Rheumatoid Arthritis
Abstract
Introduction: The PrismRA® test identifies rheumatoid arthritis (RA) patients who are unlikely to respond to anti-tumor necrosis factor (anti-TNF) therapies. This study evaluated the clinical and financial outcomes of incorporating PrismRA into routine clinical care of RA patients.
Methods: A decision-analytic model was created to evaluate clinical and economic outcomes in the 12-month period following first biologic treatment. Two treatment strategies were compared: (1) observed clinical decision-making based on a 175-patient cohort receiving an anti-TNF therapy as their first biologic after failure of conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) and (2) modeled clinical decision-making of the same population using PrismRA results to inform first-line biologic treatment choice. Modeled costs include biologic drug pharmacy, non-biologic pharmacy, and total medical costs. The odds of inadequate response to anti-TNF therapies and various components of patient care were calculated based on PrismRA results.
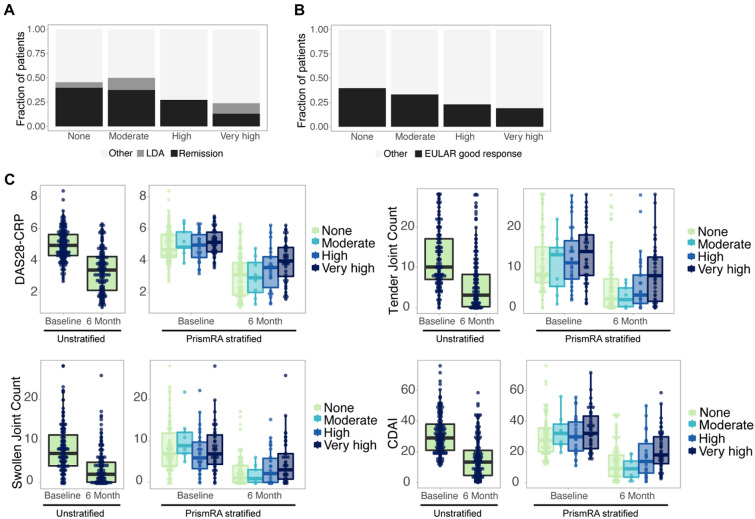
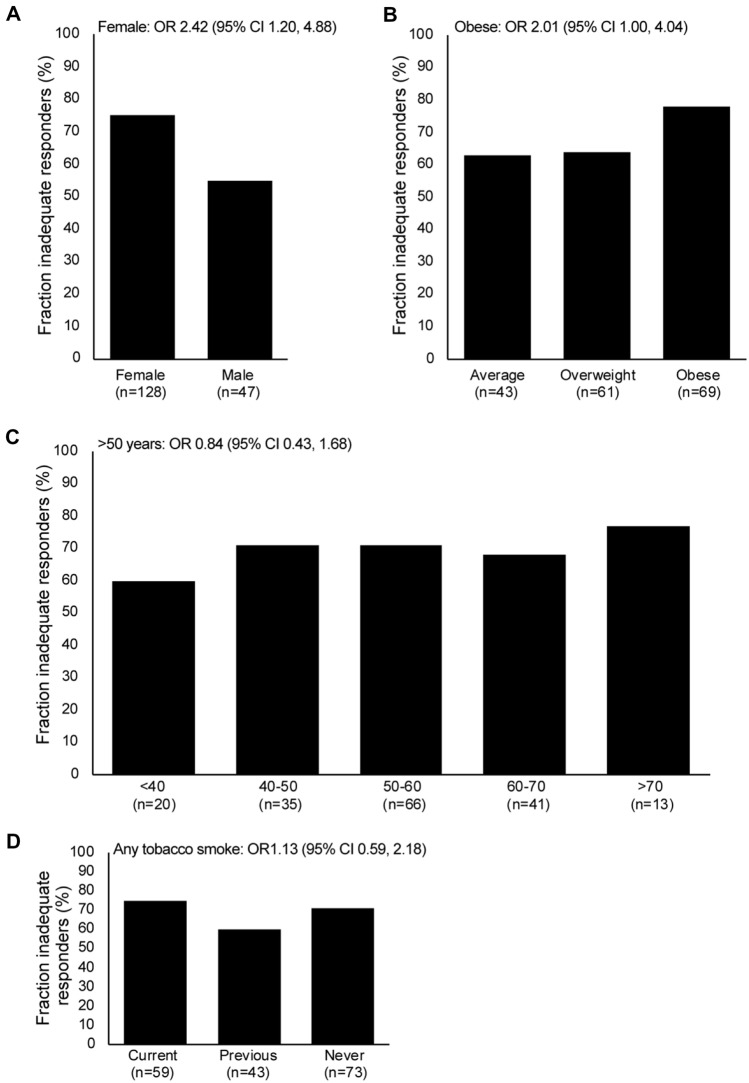
Results: Identifying predicted inadequate responders to anti-TNF therapies resulted in a modeled 38% increase in ACR50 response to first-line biologic therapies. The fraction of patients who achieved an ACR50 response to any therapy (TNFi and others) within the 12-month period was 33% higher in the PrismRA-stratified population than in the unstratified population (59 vs. 44%, respectively). When therapy prescriptions were modeled according to PrismRA results, cost savings were modeled for all financial variables: overall costs (4% decreased total, 19% decreased on ineffective treatments), total biologic drug pharmacy (4% total, 23% ineffective), non-biologic pharmacy (2% total, 19% ineffective), and medical costs (6% total, 19% ineffective). Female sex was the clinical metric that showed the greatest association with inadequate response to anti-TNF therapies (odds ratio 2.42, 95% confidence interval 1.20, 4.88).
Conclusions: If PrismRA is implemented into routine clinical care as modeled, predicting which RA patients will have an inadequate response to anti-TNF therapies could save > $7 million in overall ineffective healthcare costs per 1000 patients tested and increase targeted DMARD response rates in RA.
Keywords: Anti-TNF therapies; Budget impact; Clinical utility; Precision medicine; Rheumatoid arthritis.
Conflict of interest statement
Lixia Zhang, Anna Jeter, and Johanna B. Withers are all full-time employees of and have stock ownership in Scipher Medicine Corporation. Martin J. Bergman is a shareholder of Johnson & Johnson; has received fees as a consultant from AbbVie, Amgen, AstraZeneca, BMS, Genentech/Roche, Gilead, Janssen, Merck, Novartis, Pfizer, Regeneron, Sandoz, Sanofi; and has served as a speaker for AbbVie, Amgen, AstraZeneca, Gilead, Novartis, Regeneron, Sanofi. Alan J. Kivitz is a shareholder of Amgen, Gilead Sciences, Inc., GlaxoSmithKline, Novartis, Pfizer and Sanofi; has received fees as a consultant from AbbVie, Boehringer Ingelheim, Flexion, Gilead Sciences, Inc., Janssen, Pfizer, Regeneron, Sanofi and SUN Pharma Advanced Research; and has served as a speaker for AbbVie, Celgene, Flexion, Genzyme, Horizon, Merck, Novartis, Pfizer, Regeneron, Sanofi, and UCB. Dimitrios A. Pappas and Joel M. Kremer are employees and shareholders of CORRONA, LLC. Martin Scipher Medicine and PrismRA are trademarks of Scipher Medicine Corporation. The PrismRA predictive model is proprietary to Scipher Medicine Corporation.
Figures



References
-
- Bijlsma JWJ, Welsing PMJ, Woodworth TG, et al. Early rheumatoid arthritis treated with tocilizumab, methotrexate, or their combination (U-Act-Early): a multicentre, randomised, double-blind, double-dummy, strategy trial. Lancet. 2016;388(10042):343–355. doi: 10.1016/S0140-6736(16)30363-4. - DOI - PubMed
LinkOut - more resources
Full Text Sources
