

Clinical usefulness of fully automated chemiluminescent immunoassay for quantitative antibody measurements in COVID-19 patients
- PMID: 32797641
- PMCID: PMC7436871
- DOI: 10.1002/jmv.26430
Clinical usefulness of fully automated chemiluminescent immunoassay for quantitative antibody measurements in COVID-19 patients
Abstract
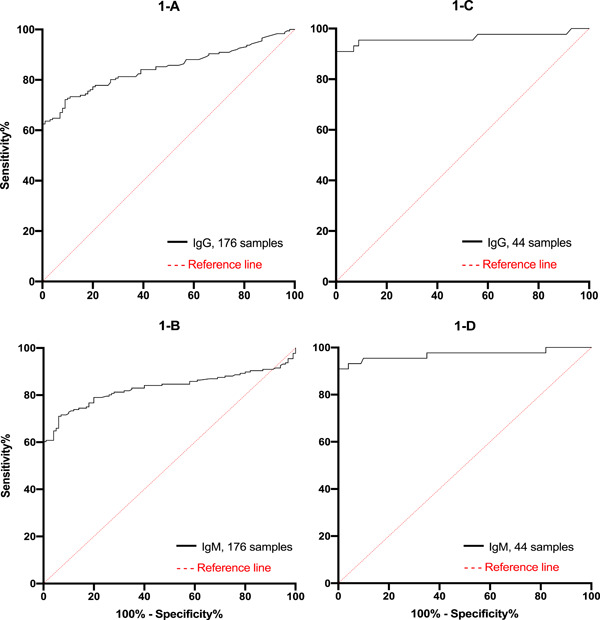
Since December 2019, we have been in the battlefield with a new threat to the humanity, known as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which causes coronavirus disease 2019 (COVID-19), characterized by viral pneumonia. It may be asymptomatic or cause various symptoms, ranging from flu-like symptoms to acute respiratory distress syndrome and eventually death. At present, the only reliable test for COVID-19 diagnosis is quantitative reverse transcriptase-polymerase chain reaction. Assessing the immune response against SARS-CoV-2 could increase the detection sensitivity of infected population. Hereby, we report the performances of a fully automated chemiluminescent immunoassay (CLIA) on 276 serum samples. One hundred samples obtained from COVID-19 negative subjects (COVID-19 free) were analyzed to evaluate the diagnostic specificity of antibody (Ab) detection. Thereafter, 176 samples obtained from 125 patients with confirmed COVID-19 (COVID-19 patients) were selected to assess the diagnostic sensitivity of the CLIA. All samples were analyzed on MAGLUMI 800 platform. All COVID-19 free samples had Ab levels below the cutoff values. Hence, the diagnostic specificity was estimated at 100% (95% confidence interval [CI] = 96.3-100.0; positive predictive value = 100%). By the 18th day from the onset of symptoms, we reached an optimal diagnostic sensitivity (more than 95.0%) In fact, the diagnostic sensitivity increased over time and between 15 and 25 days after symptoms onset, reached 95.5% (95% CI = 84.9-99.2). The new automated CLIA analyzer appeared to be a robust and reliable method to measure specific Ab against COVID-19 at high throughput. Our data suggest that combining Ab and nucleic acid detection could increase diagnostic sensitivity.
Keywords: COVID-19; Euroimmun; MAGLUMI; SARS-CoV-2; immunoassay; serology.
© 2020 Wiley Periodicals LLC.
Conflict of interest statement
The authors declare that there are no conflict of interests.
Figures
References
-
- WHO . Coronavirus Disease (COVID‐19) Pandemic 2019‐2020. Geneva, Switzerland: World Health Organization; 2020.
-
- Noordzij M, Tripepi G, Dekker FW, Zoccali C, Tanck MW, Jager KJ. Sample size calculations: basic principles and common pitfalls. Nephrol Dial Transplant. 2010;25(5):1388‐1393. - PubMed
-
- Bourner G, De la Salle B, George T, et al. ICSH guidelines for the verification and performance of automated cell counters for body fluids. Int J Lab Hematol. 2014;36(6):598‐612. - PubMed
-
- Snibe . Manufacturer's package inserts in 2019‐nCoV IgG/M‐en‐EU, V2.0. Shenzhen, China: Snibe; 2020.
-
- HAd Santé. Cahier des charges définissant les modalités d'évaluation des performances des tests sérologiques détectant les anticorps dirigés contre le SARS‐CoV‐2. Santé, France: HAd Santé; 2020.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
