

Great Expectations: A Critical Review of and Suggestions for the Study of Reward Processing as a Cause and Predictor of Depression
- PMID: 32797941
- PMCID: PMC10726343
- DOI: 10.1016/j.biopsych.2020.06.012
Great Expectations: A Critical Review of and Suggestions for the Study of Reward Processing as a Cause and Predictor of Depression
Abstract
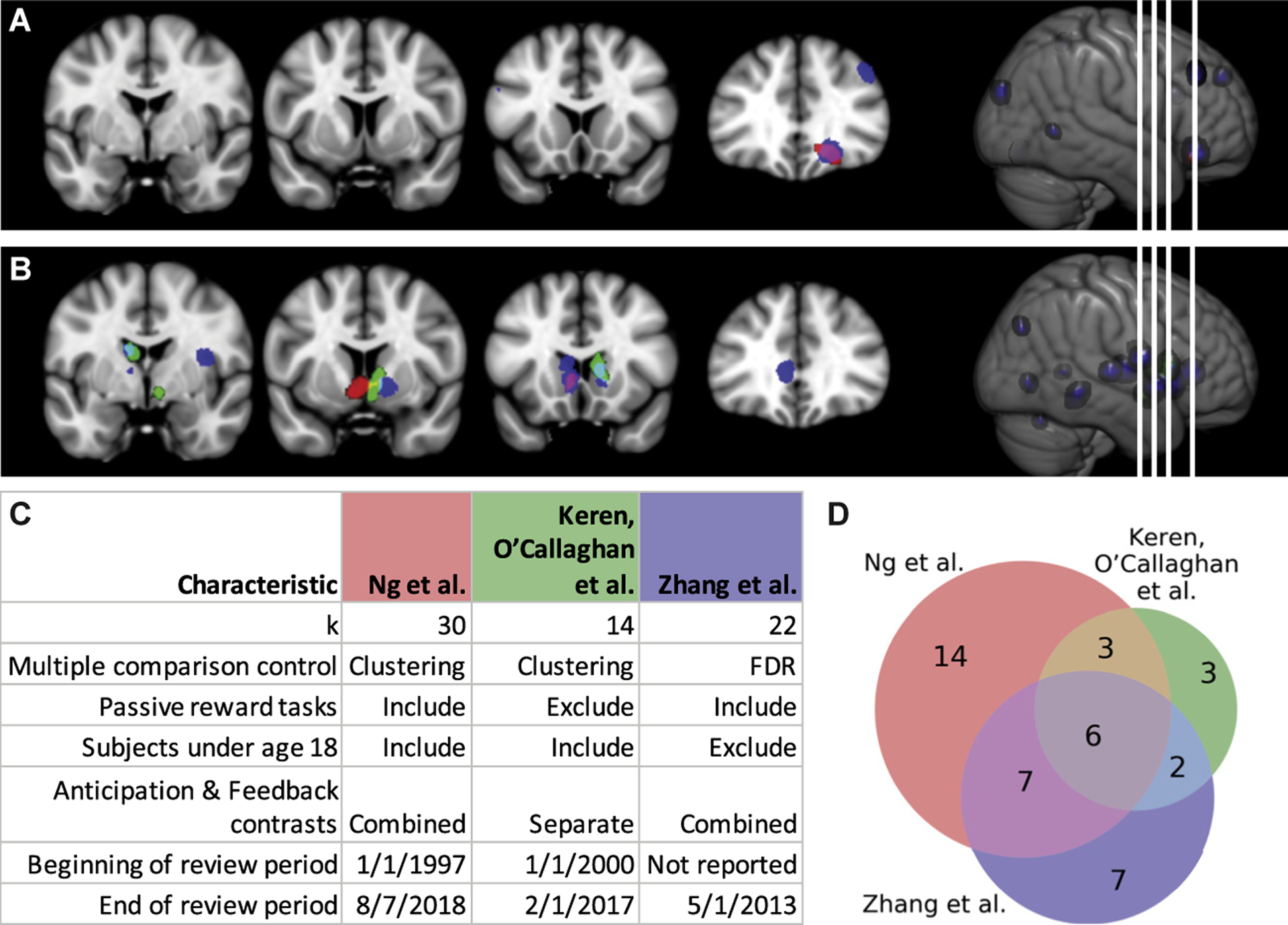
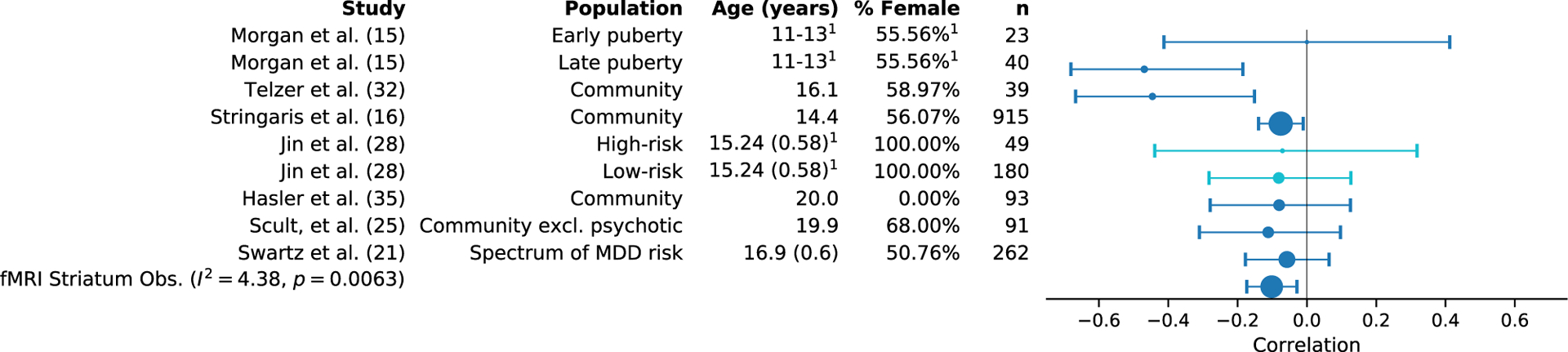
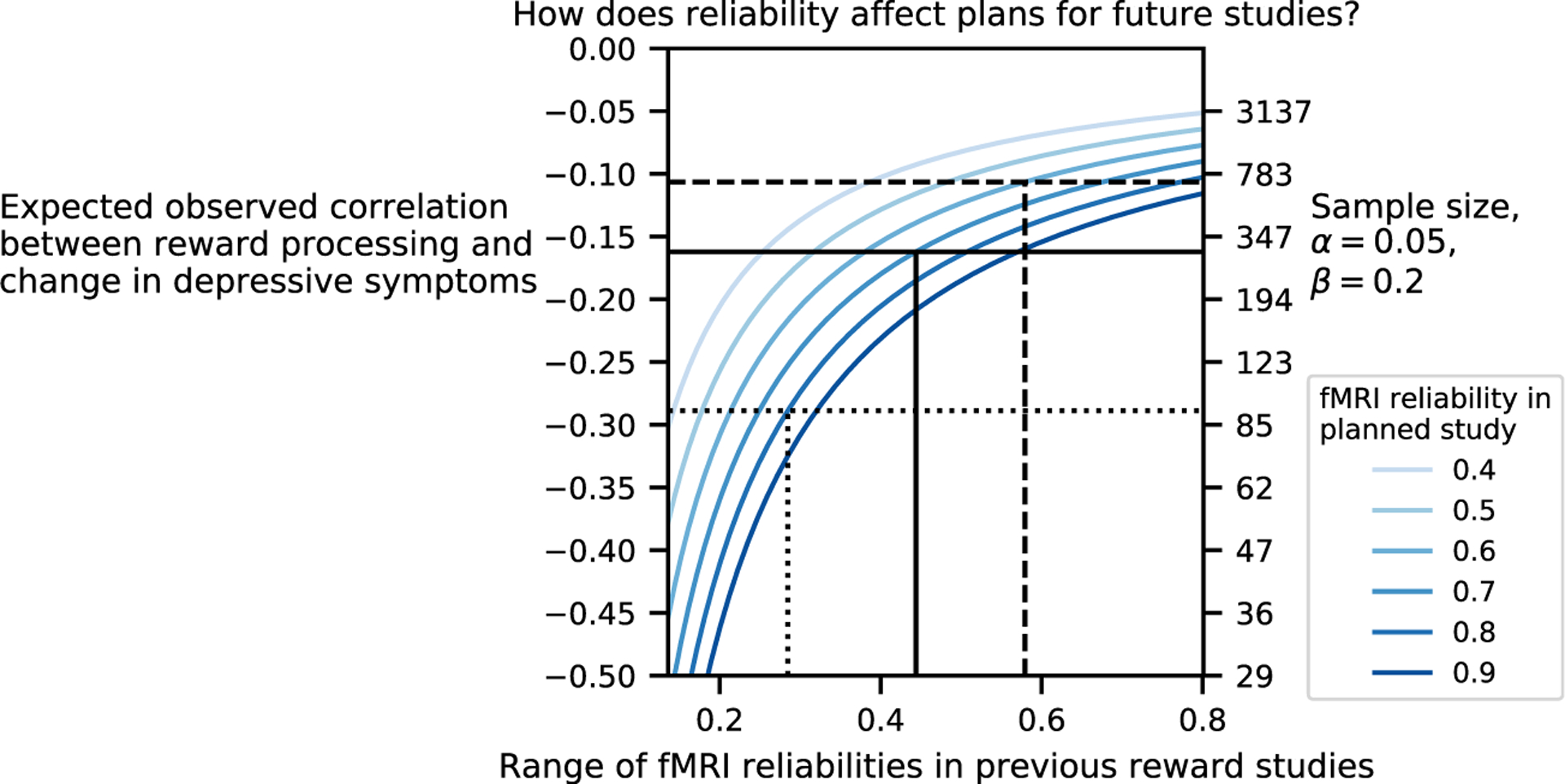
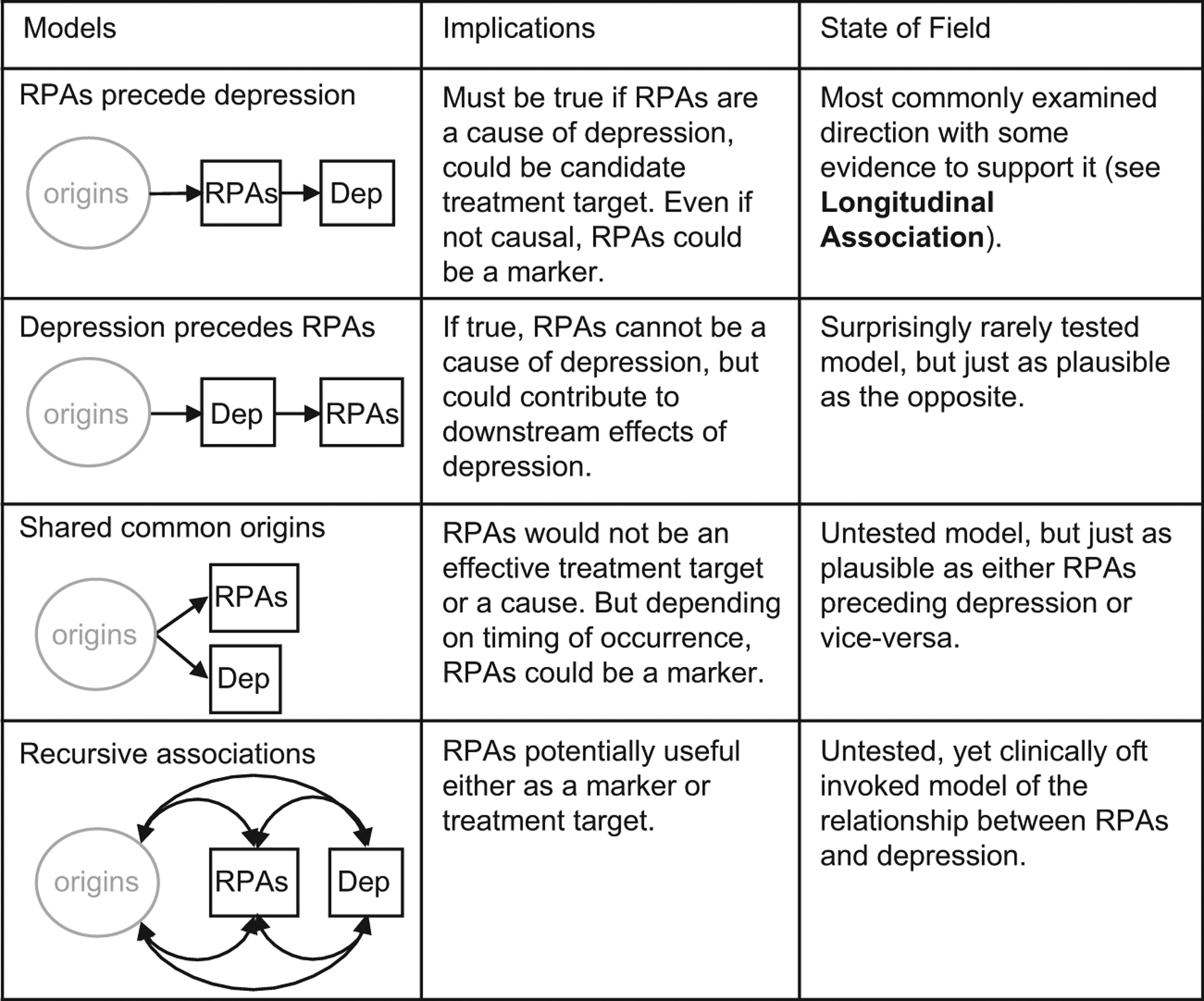
Both human and animal studies support the relationship between depression and reward processing abnormalities, giving rise to the expectation that neural signals of these processes may serve as biomarkers or mechanistic treatment targets. Given the great promise of this research line, we scrutinized those findings and the theoretical claims that underlie them. To achieve this, we applied the framework provided by classical work on causality as well as contemporary approaches to prediction. We identified a number of conceptual, practical, and analytical challenges to this line of research and used a preregistered meta-analysis to quantify the longitudinal associations between reward processing abnormalities and depression. We also investigated the impact of measurement error on reported data. We found that reward processing abnormalities do not reach levels that would be useful for clinical prediction, yet the available evidence does not preclude a possible causal role in depression.
Keywords: Depression; Development; Meta-analysis; Reliability; Reproducibility; Reward processing.
Published by Elsevier Inc.
Figures
References
-
- Haber SN (2011): Neuroanatomy of reward: A view from the ventral striatum. In: Gottfried JA, editor. Neurobiology of Sensation and Reward. Boca Raton, FL: CRC Press/Taylor & Francis, 235–261. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
