

Early postpartum physical activity and pelvic floor support and symptoms 1 year postpartum
- PMID: 32798462
- PMCID: PMC7855223
- DOI: 10.1016/j.ajog.2020.08.033
Early postpartum physical activity and pelvic floor support and symptoms 1 year postpartum
Abstract
Background: Risks of pelvic organ prolapse and urinary incontinence increase after the first vaginal delivery. During the early postpartum period, a time of active regeneration and healing of the pelvic floor, women may be particularly vulnerable to greater pelvic floor loading.
Objective: This prospective cohort study aimed to determine whether objectively measured moderate to vigorous physical activity in the early postpartum period predicts pelvic floor support and symptoms 1 year after the first vaginal birth.
Study design: We enrolled nulliparous women in the third trimester, later excluding those who had a cesarean or preterm delivery. Participants wore triaxial wrist accelerometers at 2 to 3 weeks and 5 to 6 weeks postpartum for ≥4 days. Primary outcomes, assessed 1 year postpartum, included (1) pelvic floor support on Pelvic Organ Prolapse Quantification examination, dichotomized as maximal vaginal descent of <0 cm (better support) vs ≥0 cm (worse support); and (2) pelvic floor symptom burden, considered positive with report of ≥1 bothersome symptom in ≥2 of 6 domains, assessed using the Epidemiology of Prolapse and Incontinence Questionnaire. The primary predictor was average daily moderate to vigorous physical activity. Because we could not eliminate women with pelvic floor changes before pregnancy, we modeled prevalence, rather than risk, ratios for each outcome using modified Poisson regression.
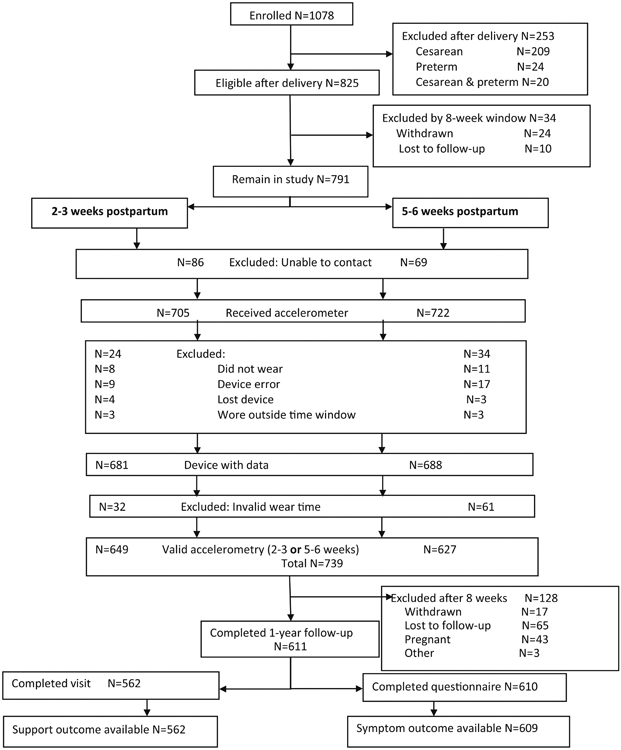
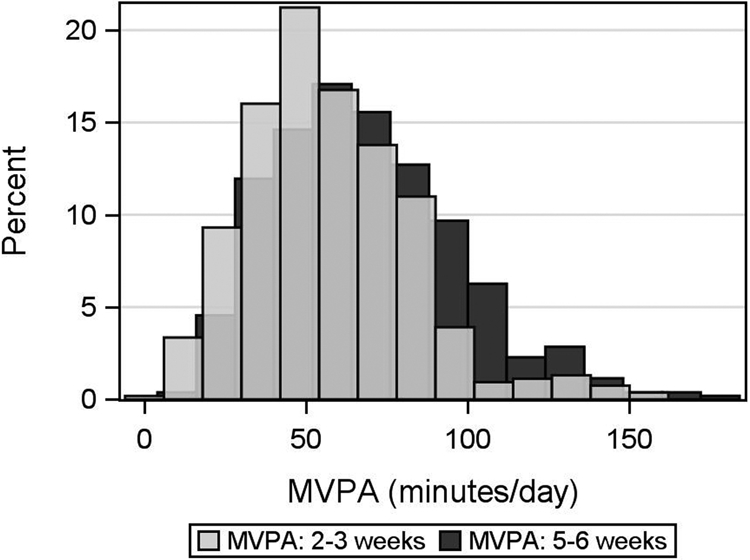
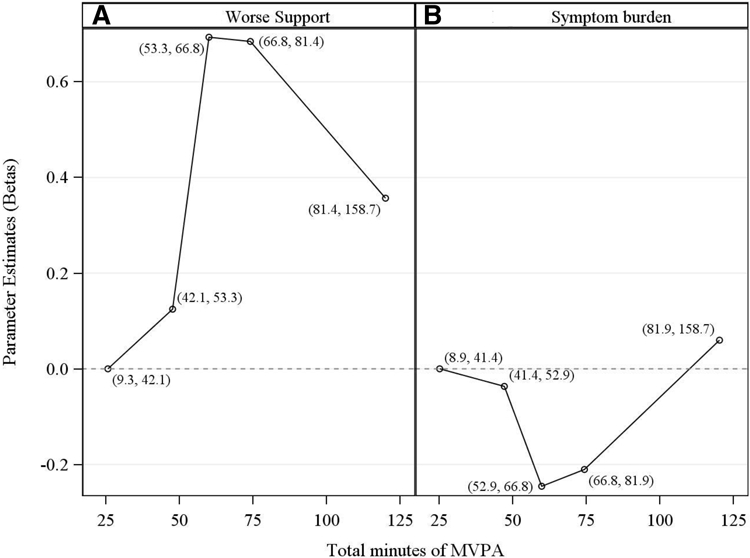
Results: Of 825 participants eligible after delivery, 611 completed accelerometry and 1-year follow-up; 562 completed in-person visits, and 609 completed questionnaires. The mean age was 28.9 years (standard deviation, 5.01). The mean for moderate to vigorous physical activity measured in minutes per day was 57.3 (standard deviation, 25.4) and 68.1 (standard deviation, 28.9) at 2 to 3 weeks and 5 to 6 weeks, respectively. One year postpartum, 53 of 562 participants (9.4%) demonstrated worse vaginal support and 330 of 609 participants (54.2%) met criteria for pelvic floor symptom burden. In addition, 324 (53.1%), 284 (46.6%), 144 (23.6%), and 25 (4.1%) reported secondary outcomes of stress urinary incontinence, overactive bladder, anal incontinence, and constipation, respectively, and 264 (43.4%), 250 (41.0%), and 89 (14.6%) reported no, mild, or moderate to severe urinary incontinence, respectively. The relationship between moderate to vigorous physical activity and outcomes was not linear. On the basis of plots, we grouped quintiles of moderate to vigorous physical activity into 3 categories: first and second quintiles combined, third and fourth quintiles combined, and fifth quintile. In final multivariable models, compared with women in moderate to vigorous physical activity quintiles 3 and 4, those in the lower 2 (prevalence ratio, 0.55; 95% confidence interval, 0.31-1.00) and upper quintile (prevalence ratio, 0.70; 95% confidence interval, 0.35-1.38)) trended toward lower prevalence of worse support. However, we observed the reverse for symptom burden: compared with women in quintiles 3 and 4, those in the lower 2 (prevalence ratio, 1.20; 95% confidence interval, 1.02-1.41) and upper quintile prevalence ratio 1.34 (95% confidence interval, 1.11-1.61) demonstrated higher prevalence of symptom burden. Moderate to vigorous physical activity did not predict any of the secondary outcomes. The presence of a delivery factor with potential to increase risk for levator ani muscle injury did not modify the effect of moderate to vigorous physical activity on outcomes.
Conclusion: Except for support, which was worse in women with moderately high levels of activity, early postpartum moderate to vigorous physical activity was either protective or had no effect on other parameters of pelvic floor health. Few women performed substantial vigorous activity, and thus, these results do not apply to women performing strenuous exercise shortly after delivery.
Keywords: accelerometry; pelvic floor disorder; pelvic organ prolapse; physical activity; postpartum; urinary incontinence.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Pelvic floor muscle strength and the incidence of pelvic floor disorders after vaginal and cesarean delivery.Am J Obstet Gynecol. 2020 Jan;222(1):62.e1-62.e8. doi: 10.1016/j.ajog.2019.08.003. Epub 2019 Aug 8. Am J Obstet Gynecol. 2020. PMID: 31422064
-
Breastfeeding and pelvic floor disorders one to two decades after vaginal delivery.Am J Obstet Gynecol. 2019 Oct;221(4):333.e1-333.e8. doi: 10.1016/j.ajog.2019.05.010. Epub 2019 May 17. Am J Obstet Gynecol. 2019. PMID: 31108062 Free PMC article.
-
Physical activity and the pelvic floor.Am J Obstet Gynecol. 2016 Feb;214(2):164-171. doi: 10.1016/j.ajog.2015.08.067. Epub 2015 Sep 6. Am J Obstet Gynecol. 2016. PMID: 26348380 Free PMC article. Review.
-
Physical and cultural determinants of postpartum pelvic floor support and symptoms following vaginal delivery: a protocol for a mixed-methods prospective cohort study.BMJ Open. 2017 Jan 10;7(1):e014252. doi: 10.1136/bmjopen-2016-014252. BMJ Open. 2017. PMID: 28073797 Free PMC article.
-
[Postpartum pelvic floor muscle training and abdominal rehabilitation: Guidelines].J Gynecol Obstet Biol Reprod (Paris). 2015 Dec;44(10):1141-6. doi: 10.1016/j.jgyn.2015.09.023. Epub 2015 Oct 31. J Gynecol Obstet Biol Reprod (Paris). 2015. PMID: 26530172 Review. French.
Cited by
-
Trends and focal points in pelvic floor reconstruction for pelvic organ prolapse: A bibliometric analysis.Medicine (Baltimore). 2024 May 10;103(19):e38131. doi: 10.1097/MD.0000000000038131. Medicine (Baltimore). 2024. PMID: 38728449 Free PMC article.
-
Strenuous physical activity, exercise, and pelvic organ prolapse: a narrative scoping review.Int Urogynecol J. 2023 Jun;34(6):1153-1164. doi: 10.1007/s00192-023-05450-3. Epub 2023 Jan 24. Int Urogynecol J. 2023. PMID: 36692525 Free PMC article.
-
Effect of Pelvic Floor Workout on Pelvic Floor Muscle Function Recovery of Postpartum Women: Protocol for a Randomized Controlled Trial.Int J Environ Res Public Health. 2022 Sep 4;19(17):11073. doi: 10.3390/ijerph191711073. Int J Environ Res Public Health. 2022. PMID: 36078788 Free PMC article.
-
Pelvic Floor Support and Symptoms 1 Year Postpartum in Relation to Excess Body Habitus Before, During and After First Vaginal Birth.Female Pelvic Med Reconstr Surg. 2022 May 1;28(5):273-279. doi: 10.1097/SPV.0000000000001150. Epub 2022 Feb 16. Female Pelvic Med Reconstr Surg. 2022. PMID: 35234181 Free PMC article.
-
Postpartum sedentary behaviour and pelvic floor support: A prospective cohort study.J Sports Sci. 2023 Jan;41(2):141-150. doi: 10.1080/02640414.2023.2202063. Epub 2023 Apr 13. J Sports Sci. 2023. PMID: 37055921 Free PMC article.
References
-
- Smith FJ, Holman CD, Moorin RE, Tsokos N. Lifetime risk of undergoing surgery for pelvic organ prolapse. Obstet Gynecol. 2010;116(5):1096–1100. - PubMed
-
- Løwenstein E, Ottesen B, Gimbel H. Incidence and lifetime risk of pelvic organ prolapse surgery in Denmark from 1977 to 2009. Int Urogynecol J. 2014. - PubMed
-
- Risk factors for genital prolapse in non-hysterectomized women around menopause. Results from a large cross-sectional study in menopausal clinics in Italy. Progetto Menopausa Italia Study Group. Eur J Obstet Gynecol Reprod Biol. 2000;93(2):135–140. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
