

Paramagnetic Rim Lesions are Specific to Multiple Sclerosis: An International Multicenter 3T MRI Study
- PMID: 32799417
- PMCID: PMC9943711
- DOI: 10.1002/ana.25877
Paramagnetic Rim Lesions are Specific to Multiple Sclerosis: An International Multicenter 3T MRI Study
Abstract
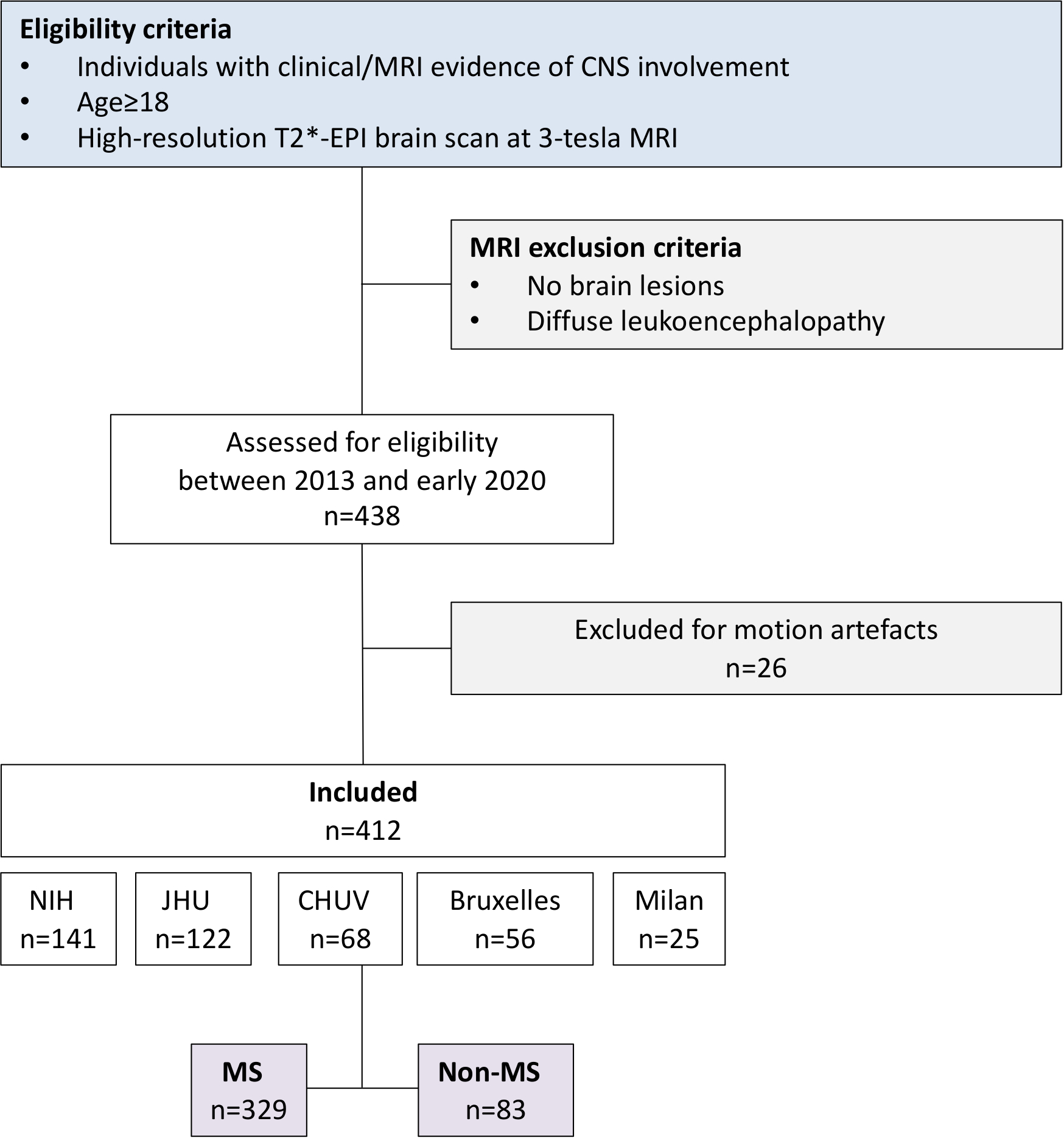
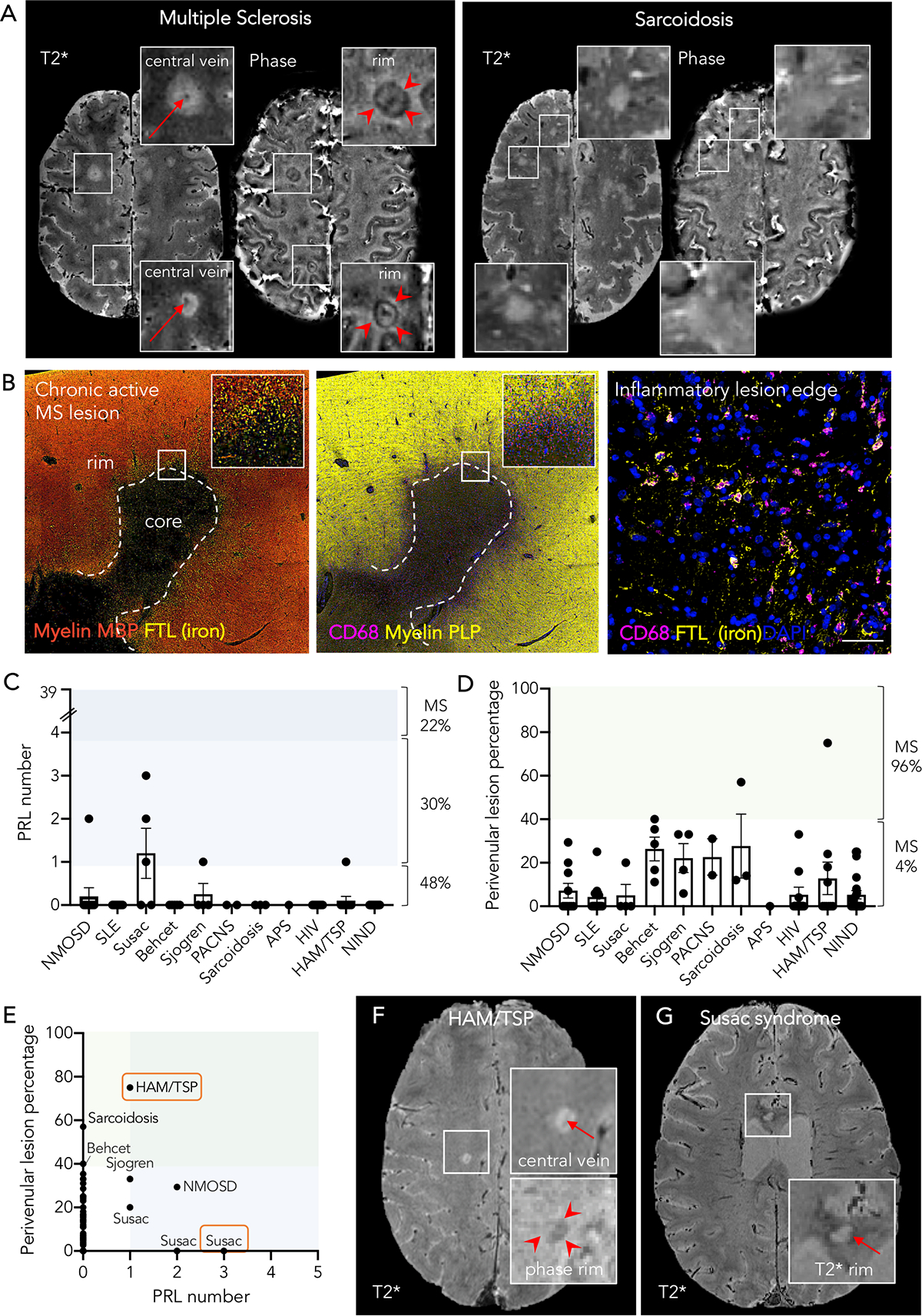
In multiple sclerosis (MS), a subset of chronic active white matter lesions are identifiable on magnetic resonance imaging by their paramagnetic rims, and increasing evidence supports their association with severity of clinical disease. We studied their potential role in differential diagnosis, screening an international multicenter clinical research-based sample of 438 individuals affected by different neurological conditions (MS, other inflammatory, infectious, and non-inflammatory conditions). Paramagnetic rim lesions, rare in other neurological conditions (52% of MS vs 7% of non-MS cases), yielded high specificity (93%) in differentiating MS from non-MS. Future prospective multicenter studies should validate their role as a diagnostic biomarker. ANN NEUROL 2020;88:1034-1042.
© 2020 American Neurological Association.
Conflict of interest statement
Potential Conflicts of Interest
Nothing to report.
Figures
References
-
- Solomon AJ, Corboy JR. The tension between early diagnosis and misdiagnosis of multiple sclerosis. Nat Rev Neurol 2017;13:567–572. - PubMed
-
- Kaisey M, Solomon AJ, Luu M, Giesser BS, Sicotte NL. Incidence of multiple sclerosis misdiagnosis in referrals to two academic centers. Mult Scler Relat Disord 2019;30:51–56. - PubMed
-
- Mistry N, Dixon J, Tallantyre E, et al. Central veins in brain lesions visualized with high-field magnetic resonance imaging: a pathologically specific diagnostic biomarker for inflammatory demyelination in the brain. JAMA Neurol 2013;70:623–628. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
