

Cost-Effectiveness of Operating on Traumatic Spinal Injuries in Low-Middle Income Countries: A Preliminary Report From a Major East African Referral Center
- PMID: 32799677
- PMCID: PMC8965297
- DOI: 10.1177/2192568220944888
Cost-Effectiveness of Operating on Traumatic Spinal Injuries in Low-Middle Income Countries: A Preliminary Report From a Major East African Referral Center
Abstract
Study design: Retrospective cost-effectiveness analysis.
Objectives: While the incidence of traumatic spine injury (TSI) is high in low-middle income countries (LMICs), surgery is rarely possible due to cost-prohibitive implants. The objective of this study was to conduct a preliminary cost-effectiveness analysis of operative treatment of TSI patients in a LMIC setting.
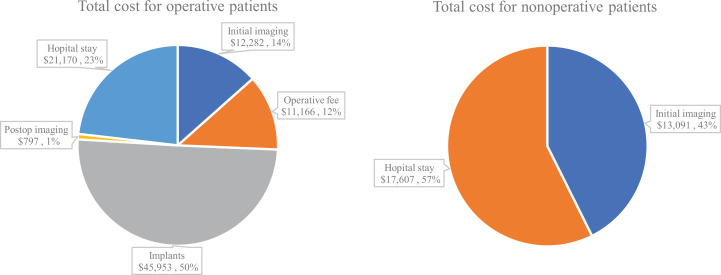
Methods: At a tertiary hospital in Tanzania from September 2016 to May 2019, a retrospective analysis was conducted to estimate the cost-effectiveness of operative versus nonoperative treatment of TSI. Operative treatment included decompression/stabilization. Nonoperative treatment meant 3 months of bed rest. Direct costs included imaging, operating fees, surgical implants, and length of stay. Four patient scenarios were chosen to represent the heterogeneity of spine trauma: Quadriplegic, paraplegic, neurologic improvement, and neurologically intact. Disability-adjusted-life-years (DALYs) and incremental-cost-effectiveness ratios were calculated to determine the cost per unit benefit of operative versus nonoperative treatment. Cost/DALY averted was the primary outcome (i.e., the amount of money required to avoid losing 1 year of healthy life).
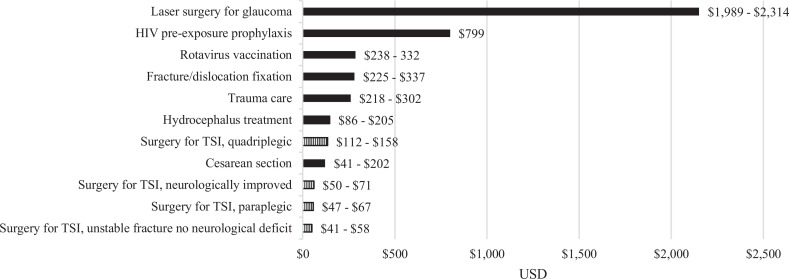
Results: A total of 270 TSI patients were included (125 operative; 145 nonoperative). Operative treatment averaged $731/patient. Nonoperative care averaged $212/patient. Comparing operative versus nonoperative treatment, the incremental cost/DALY averted for each patient outcome was: quadriplegic ($112-$158/DALY averted), paraplegic ($47-$67/DALY averted), neurologic improvement ($50-$71/DALY averted), neurologically intact ($41-$58/DALY averted). Sensitivity analysis confirmed these findings without major differences.
Conclusions: This preliminary cost-effectiveness analysis suggests that the upfront costs of spine trauma surgery may be offset by a reduction in disability. LMIC governments should consider conducting more spine trauma cost-effectiveness analyses and including spine trauma surgery in universal health care.
Keywords: East Africa; Tanzania; global neurosurgery; low-middle income countries; neurotrauma; traumatic spinal cord injury.
Conflict of interest statement
Figures
References
LinkOut - more resources
Full Text Sources
