

Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) and coronavirus disease 19 (COVID-19) - anatomic pathology perspective on current knowledge
- PMID: 32799894
- PMCID: PMC7427697
- DOI: 10.1186/s13000-020-01017-8
Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) and coronavirus disease 19 (COVID-19) - anatomic pathology perspective on current knowledge
Abstract
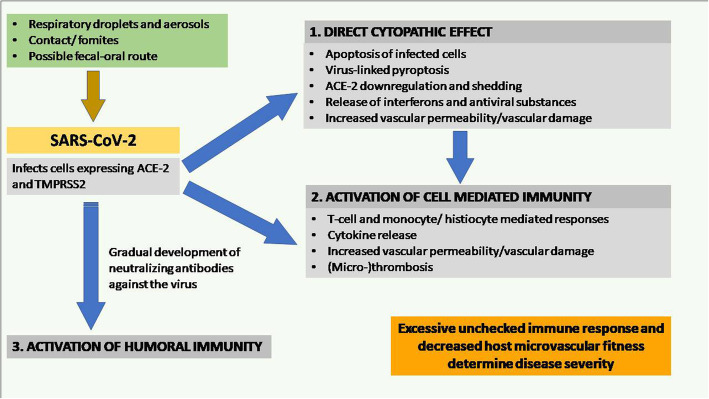
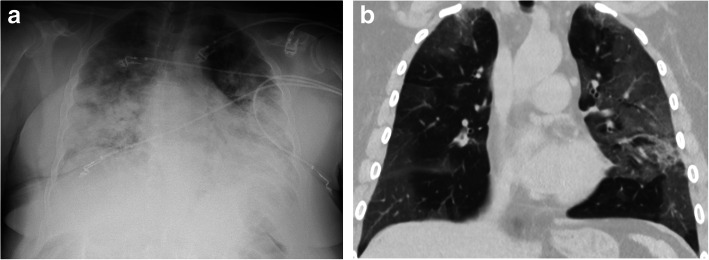
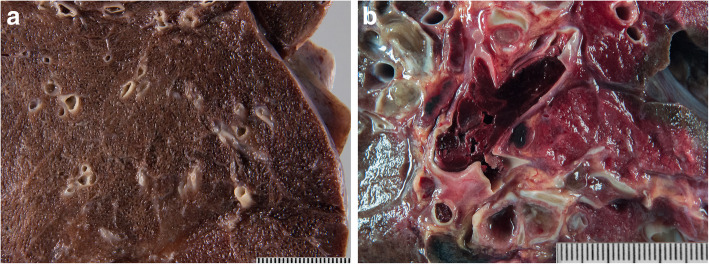
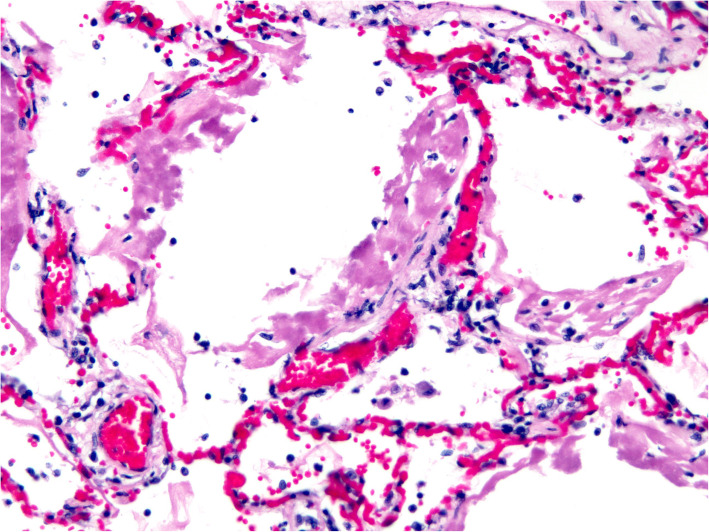
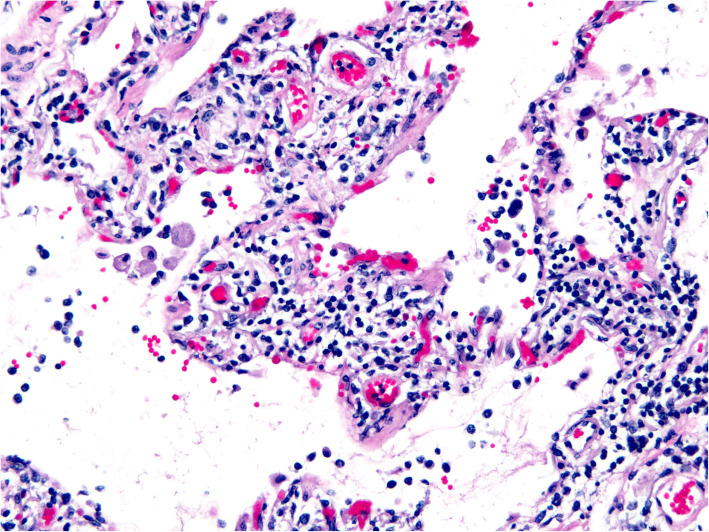
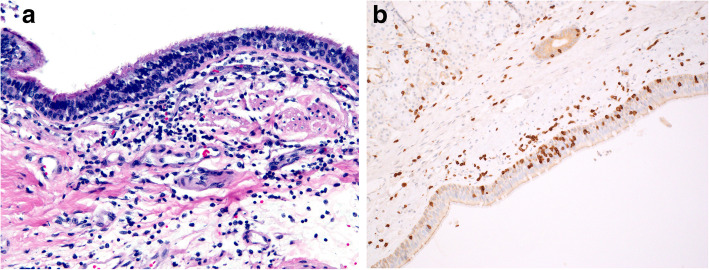
Background: The world is currently witnessing a major devastating pandemic of Coronavirus disease-2019 (COVID-19). This disease is caused by a novel coronavirus named Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2). It primarily affects the respiratory tract and particularly the lungs. The virus enters the cell by attaching its spike-like surface projections to the angiotensin-converting enzyme-2 (ACE-2) expressed in various tissues. Though the majority of symptomatic patients have mild flu-like symptoms, a significant minority develop severe lung injury with acute respiratory distress syndrome (ARDS), leading to considerable morbidity and mortality. Elderly patients with previous cardiovascular comorbidities are particularly susceptible to severe clinical manifestations. BODY: Currently, our limited knowledge of the pathologic findings is based on post-mortem biopsies, a few limited autopsies, and very few complete autopsies. From these reports, we know that the virus can be found in various organs but the most striking tissue damage involves the lungs resulting almost always in diffuse alveolar damage with interstitial edema, capillary congestion, and occasional interstitial lymphocytosis, causing hypoxia, multiorgan failure, and death. A few pathology studies have also reported intravascular microthrombi and pulmonary thrombembolism. Although the clinical presentation of this disease is fairly well characterized, knowledge of the pathologic aspects remains comparatively limited.
Conclusion: In this review, we discuss clinical, pathologic, and genomic features of COVID-19, review current hypotheses regarding the pathogenesis, and briefly discuss the clinical characteristics. We also compare the salient features of COVID-19 with other coronavirus-related illnesses that have posed significant public health issues in the past, including SARS and the Middle East Respiratory Syndrome (MERS).
Keywords: Autopsy; COVID-19; Pathogenesis; Pathology.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
