

Management of the Nasal Deformity in the Unilateral Cleft of the Lip and Nose
- PMID: 32801524
- PMCID: PMC7410885
- DOI: 10.1007/s12663-020-01412-0
Management of the Nasal Deformity in the Unilateral Cleft of the Lip and Nose
Abstract
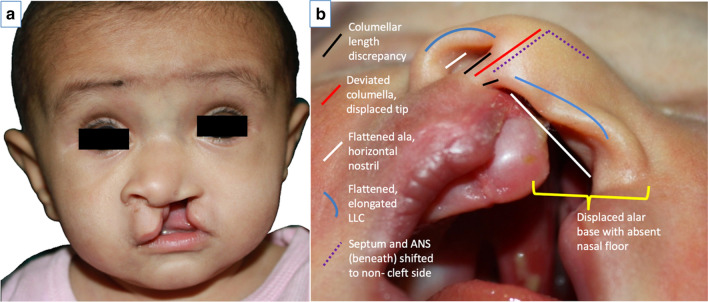
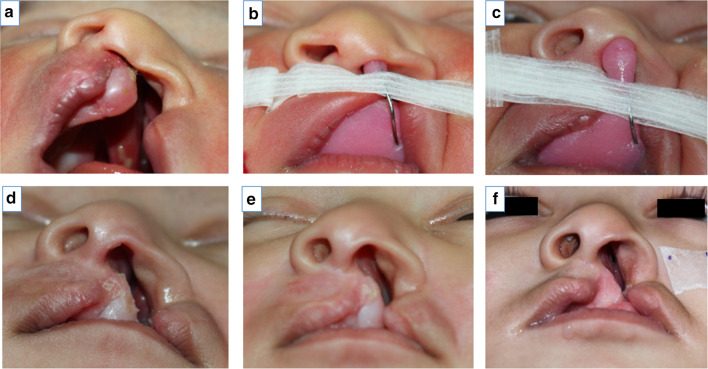
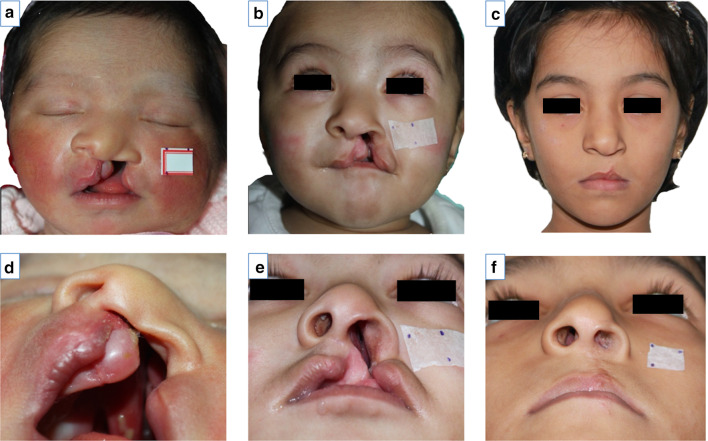
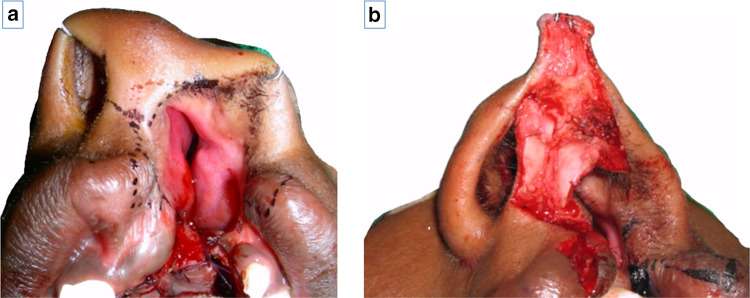
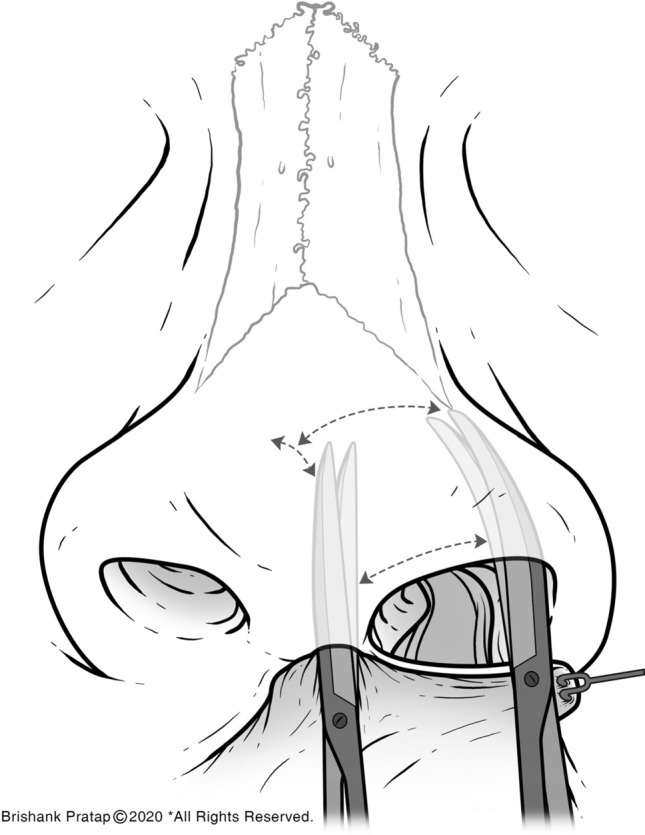
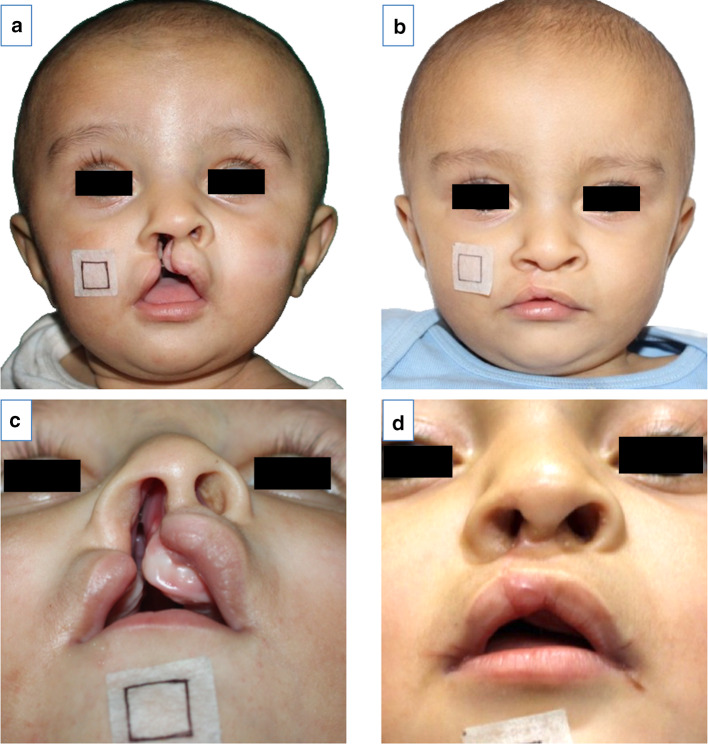
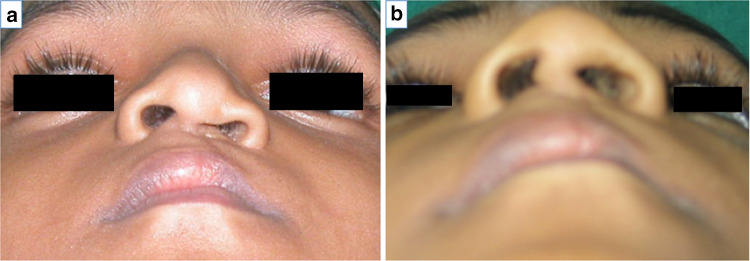
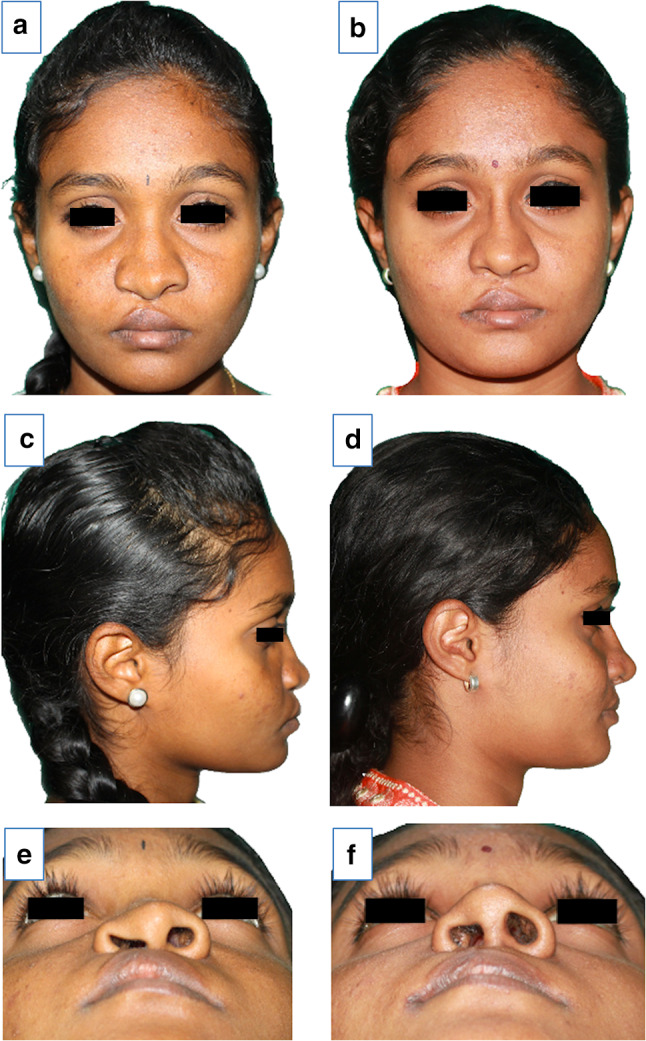
Cleft rhinoplasty is a demanding, technique-sensitive procedure. Part art, part science; it poses several probing questions to the surgeon. The unilateral cleft nasal deformity is a distinct entity because the pursuit of symmetry in the unilateral cleft nose makes the repair much more challenging. The advent of nasoalveolar moulding, the gaining popularity of primary (early) nasal repair and greater refinements in secondary (definitive) rhinoplasty techniques have contributed to better nasal results in unilateral cleft repair. Yet, some obstacles remain. This paper aims to discuss the anatomy of the unilateral cleft nose, enumerate aims and objectives of repair at every stage, and to demonstrate the evolution and varied rationale of management of nasal deformities in the unilateral cleft lip and nose.
Keywords: Cleft nasal deformity; Cleft rhinoplasty; Unilateral cleft lip; Unilateral cleft nose.
© The Association of Oral and Maxillofacial Surgeons of India 2020.
Figures

Similar articles
-
Alar web in cleft lip nose deformity: study in adult unilateral clefts.J Craniofac Surg. 2012 Sep;23(5):1349-54. doi: 10.1097/SCS.0b013e31826467e5. J Craniofac Surg. 2012. PMID: 22948620
-
Cleft rhinoplasty.J Pharm Bioallied Sci. 2015 Aug;7(Suppl 2):S691-4. doi: 10.4103/0975-7406.163480. J Pharm Bioallied Sci. 2015. PMID: 26538945 Free PMC article.
-
Primary definitive nasal correction in patients presenting for late unilateral cleft lip repair.Plast Reconstr Surg. 2002 Jul;110(1):17-24. doi: 10.1097/00006534-200207000-00005. Plast Reconstr Surg. 2002. PMID: 12087225
-
Secondary cleft rhinoplasty.JAMA Facial Plast Surg. 2014 Jan-Feb;16(1):58-63. doi: 10.1001/jamafacial.2013.1562. JAMA Facial Plast Surg. 2014. PMID: 24201895 Review.
-
Cleft Septorhinoplasty: Form and Function.Facial Plast Surg Clin North Am. 2017 May;25(2):223-238. doi: 10.1016/j.fsc.2016.12.011. Facial Plast Surg Clin North Am. 2017. PMID: 28340653 Review.
Cited by
-
Surgical design and application of alar cartilage positioning and repositioning in correcting cleft lip nose deformity.Hua Xi Kou Qiang Yi Xue Za Zhi. 2022 Mar 25;40(2):134-138. doi: 10.7518/hxkq.2022.02.002. Hua Xi Kou Qiang Yi Xue Za Zhi. 2022. PMID: 38597044 Free PMC article. Chinese, English.
-
Rhinoplasty Exclusively Utilizing Autologous Costal Cartilage for Patients with Prior Unilateral Cleft Lip Repair.Plast Reconstr Surg Glob Open. 2024 Jul 1;12(7):e5941. doi: 10.1097/GOX.0000000000005941. eCollection 2024 Jul. Plast Reconstr Surg Glob Open. 2024. PMID: 38957724 Free PMC article.
-
Egyptian patients with cleft lip: our experience with primary rhinoplasty.Maxillofac Plast Reconstr Surg. 2024 Nov 4;46(1):36. doi: 10.1186/s40902-024-00448-3. Maxillofac Plast Reconstr Surg. 2024. PMID: 39489830 Free PMC article.
-
Thermographic analysis of postoperative changes in the nasal breathing efficiency in infants and young children with unilateral cleft lip.Int J Comput Assist Radiol Surg. 2021 Dec;16(12):2225-2234. doi: 10.1007/s11548-021-02496-w. Epub 2021 Oct 8. Int J Comput Assist Radiol Surg. 2021. PMID: 34625871
-
The Four-line Algorithm for the Treatment of Unilateral Cleft Lip.Plast Reconstr Surg Glob Open. 2025 Feb 7;13(2):e6529. doi: 10.1097/GOX.0000000000006529. eCollection 2025 Feb. Plast Reconstr Surg Glob Open. 2025. PMID: 39925472 Free PMC article.
References
-
- Blair VP, Brown JB. Nasal abnormalities, fancied and real. Int J Orthod Oral Surg Radiogr. 1932;18:363–401. doi: 10.1016/s0099-6963(32)80076-1. - DOI
Publication types
LinkOut - more resources
Full Text Sources