

Outcomes and Adverse Effects of Deep Brain Stimulation on the Ventral Intermediate Nucleus in Patients with Essential Tremor
- PMID: 32802034
- PMCID: PMC7416257
- DOI: 10.1155/2020/2486065
Outcomes and Adverse Effects of Deep Brain Stimulation on the Ventral Intermediate Nucleus in Patients with Essential Tremor
Abstract
Objective: This study was aimed at identifying the potential outcome predictors, comparing the efficacy in patients with different tremor characteristics, and summarizing the adverse effect rates (AERs) of deep brain stimulation on the ventral intermediate nucleus (VIM-DBS) for essential tremor (ET).
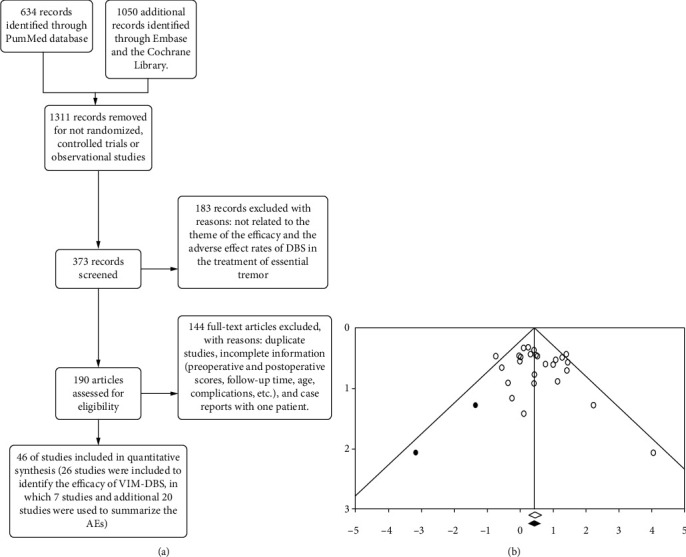
Methods: An extensive search of articles published to date in 2019 was conducted, and two main aspects were analyzed. Improvement was calculated as a percentage of change in any objective tremor rating scale (TRS) and analyzed by subgroup analyses of patients' tremor characteristics, laterality, and stimulation parameters. Furthermore, the AERs were analyzed as follows: the adverse effects (AEs) were classified as stimulation-related, surgical-related, or device-related effects. A simple regression analysis was used to identify the potential prognostic factors, and a two-sample mean-comparison test was used to verify the statistical significance of the subgroup analyses.
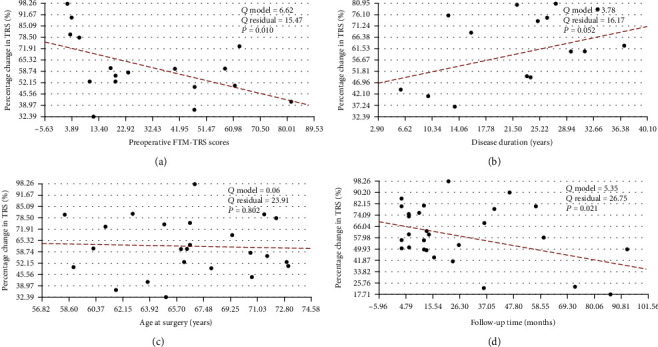
Results: Forty-six articles involving 1714 patients were included in the meta-analysis. The pooled improvement in any objective TRS score was 61.3% (95% CI: 0.564-0.660) at the mean follow-up visit (20.0 ± 17.3 months). The midline and extremity symptoms showed consistent improvement (P = 0.440), and the results of the comparison of postural and kinetic tremor were the same (P = 0.219). In addition, the improvement in rest tremor was similar to that in action tremor (OR = 2.759, P = 0.120). In the simple regression analysis, the preoperative Fahn-Tolosa-Marin Tremor Rating Scale (FTM-TRS) scores and follow-up time were negatively correlated with the percentage change in any objective TRS score (P < 0.05). The most common adverse event was dysarthria (10.5%), which is a stimulation-related AE (23.6%), while the rates of the surgical-related and device-related AEs were 6.4% and 11.5%, respectively.
Conclusion: VIM-DBS is an efficient and safe surgical method in ET, and the efficacy was not affected by the body distribution of tremor, age at surgery, and disease duration. Lower preoperative FTM-TRS scores likely indicate greater improvement, and the effect of VIM-DBS declines over time.
Copyright © 2020 Guohui Lu et al.
Conflict of interest statement
The authors report no conflicts of interest concerning the materials or methods used in this study or the findings specified in this paper.
Figures
Similar articles
-
Structural connectivity-based segmentation of the thalamus and prediction of tremor improvement following thalamic deep brain stimulation of the ventral intermediate nucleus.Neuroimage Clin. 2018;20:1266-1273. doi: 10.1016/j.nicl.2018.10.009. Epub 2018 Oct 10. Neuroimage Clin. 2018. PMID: 30318403 Free PMC article.
-
Loss of long-term benefit from VIM-DBS in essential tremor: A secondary analysis of repeated measurements.CNS Neurosci Ther. 2022 Feb;28(2):279-288. doi: 10.1111/cns.13770. Epub 2021 Dec 5. CNS Neurosci Ther. 2022. PMID: 34866345 Free PMC article.
-
Longitudinal follow-up with VIM thalamic deep brain stimulation for dystonic or essential tremor.Neurology. 2020 Mar 10;94(10):e1073-e1084. doi: 10.1212/WNL.0000000000008875. Epub 2020 Feb 11. Neurology. 2020. PMID: 32047071 Free PMC article.
-
Reduction in DBS frequency improves balance difficulties after thalamic DBS for essential tremor.J Neurol Sci. 2016 Aug 15;367:122-7. doi: 10.1016/j.jns.2016.06.001. Epub 2016 Jun 2. J Neurol Sci. 2016. PMID: 27423573 Review.
-
Deep brain stimulation and essential tremor.J Clin Neurophysiol. 2004 Jan-Feb;21(1):2-5. doi: 10.1097/00004691-200401000-00002. J Clin Neurophysiol. 2004. PMID: 15097289 Review.
Cited by
-
T-type calcium channels as therapeutic targets in essential tremor and Parkinson's disease.Ann Clin Transl Neurol. 2023 Apr;10(4):462-483. doi: 10.1002/acn3.51735. Epub 2023 Feb 4. Ann Clin Transl Neurol. 2023. PMID: 36738196 Free PMC article. Review.
-
Interim Safety Profile From the Feasibility Study of the BrainGate Neural Interface System.Neurology. 2023 Mar 14;100(11):e1177-e1192. doi: 10.1212/WNL.0000000000201707. Epub 2023 Jan 13. Neurology. 2023. PMID: 36639237 Free PMC article. Clinical Trial.
-
High-intensity focused ultrasound (HIFU) versus deep brain stimulation (DBS) for refractory tremor: team HIFU.Arq Neuropsiquiatr. 2025 Jul;83(7):1-4. doi: 10.1055/s-0045-1809660. Epub 2025 Jul 17. Arq Neuropsiquiatr. 2025. PMID: 40675616 Free PMC article. Review.
-
Deep brain stimulation for neurological disorders: a protocol for a systematic review with meta-analysis and Trial Sequential Analysis of randomised clinical trials.Syst Rev. 2022 Oct 13;11(1):218. doi: 10.1186/s13643-022-02095-z. Syst Rev. 2022. PMID: 36229825 Free PMC article.
-
Management of essential tremor deep brain stimulation-induced side effects.Front Hum Neurosci. 2024 Feb 22;18:1353150. doi: 10.3389/fnhum.2024.1353150. eCollection 2024. Front Hum Neurosci. 2024. PMID: 38454907 Free PMC article. Review.
References
-
- Zesiewicz T. A., Elble R., Louis E. D., et al. Practice parameter: therapies for essential tremor: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2005;64(12):2008–2020. doi: 10.1212/01.WNL.0000163769.28552.CD. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
