

Synchronous Abdominal Wall and Small-bowel Transplantation: A 1-year Follow-up
- PMID: 32802681
- PMCID: PMC7413814
- DOI: 10.1097/GOX.0000000000002995
Synchronous Abdominal Wall and Small-bowel Transplantation: A 1-year Follow-up
Abstract
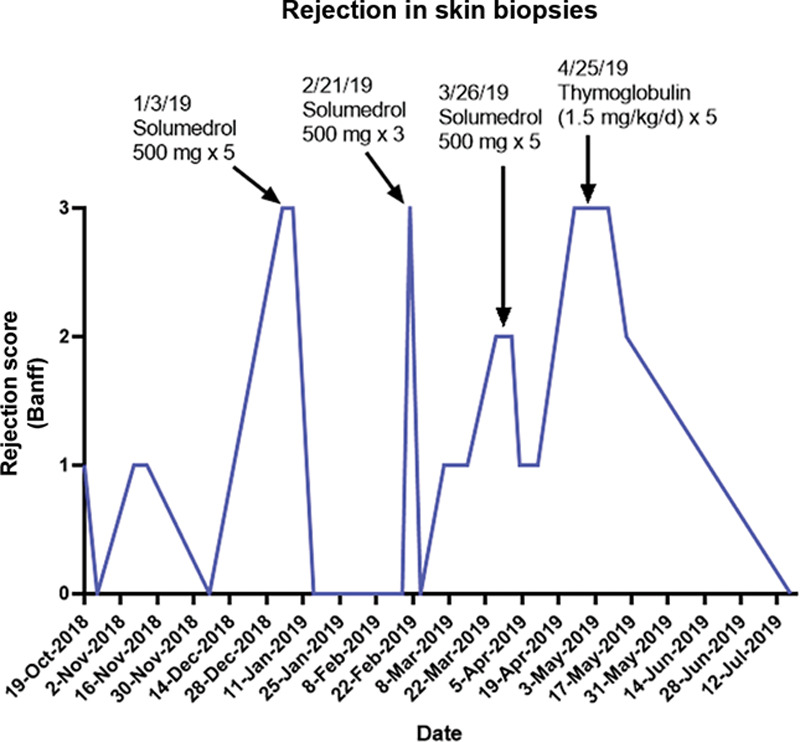
Abdominal wall-vascularized composite allotransplantation (AW-VCA) has evolved as a technically feasible but challenging option in the rare event of abdominal wall reconstruction in patients whose abdomen cannot be closed by applying conventional methods. The authors conducted the first synchronous child-to-adult recipient AW-VCA using an arteriovenous loop technique. This article presents a 1-year follow-up of the patient's postoperative course. Frequent skin biopsies were performed in accordance with Duke Institutional Review Board protocol, with 3 episodes of rejection treated with high-dose steroids and Thymoglobulin (Genzyme Corp, Cambridge, Mass.). The patient developed an opportunistic fungal brain abscess secondary to immunosuppression, which led to temporary upper extremity weakness. Future considerations for AW-VCA include a modified surgical technique involving utilization of donor vein graft for arteriovenous loop formation. In addition, reduction in postoperative biopsy schedule and changes in immunosuppression regimen may lead to improved outcomes and prevent unnecessary high-dose immunosuppression.
Copyright © 2020 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Figures








References
-
- Levi DM, Tzakis AG, Kato T, et al. Transplantation of the abdominal wall. Lancet. 2003;361:2173–2176. - PubMed
-
- Light D, Kundu N, Djohan R, et al. Total abdominal wall transplantation: an anatomical study and classification system. Plast Reconstr Surg. 2017;139:1466–1473. - PubMed
-
- Giele H, Vaidya A, Reddy S, et al. Current state of abdominal wall transplantation. Curr Opin Organ Transplant. 2016;21:159–164. - PubMed
-
- Carlsen BT, Farmer DG, Busuttil RW, et al. Incidence and management of abdominal wall defects after intestinal and multivisceral transplantation. Plast Reconstr Surg. 2007;119:1247–1255; discussion 1256. - PubMed
-
- Alexandrides IJ, Liu P, Marshall DM, et al. Abdominal wall closure after intestinal transplantation. Plast Reconstr Surg. 2000;106:805–812. - PubMed
LinkOut - more resources
Full Text Sources