

Antihypertensive medications ameliorate Alzheimer's disease pathology by slowing its propagation
- PMID: 32802934
- PMCID: PMC7424255
- DOI: 10.1002/trc2.12060
Antihypertensive medications ameliorate Alzheimer's disease pathology by slowing its propagation
Abstract
Introduction: Mounting evidence supports an association between antihypertensive medication use and reduced risk of Alzheimer's disease (AD). Consensus on possible pathological mechanisms remains elusive.
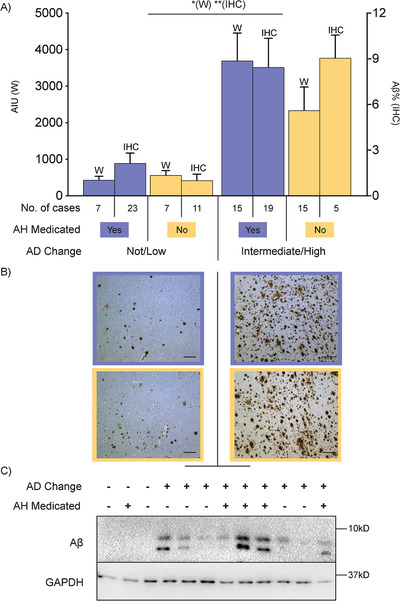
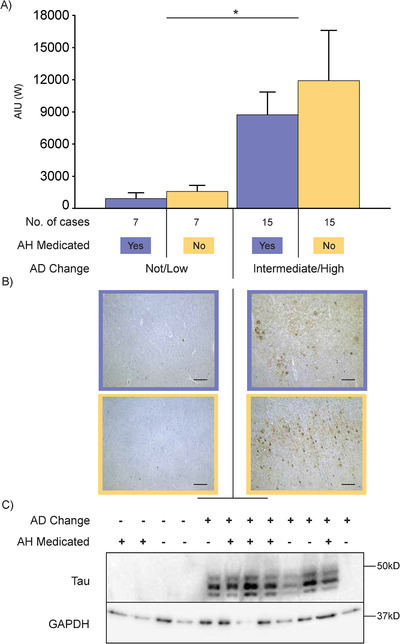
Methods: Human brain tissue from a cohort followed to autopsy that included 96 cases of AD (46 medicated for hypertension) and 53 pathological controls (33 also medicated) matched for cerebrovascular disease was available from the New South Wales Brain Banks. Quantified frontal cortex amyloid beta (Aβ) and tau proteins plus Alzheimer's neuropathologic change scores were analyzed.
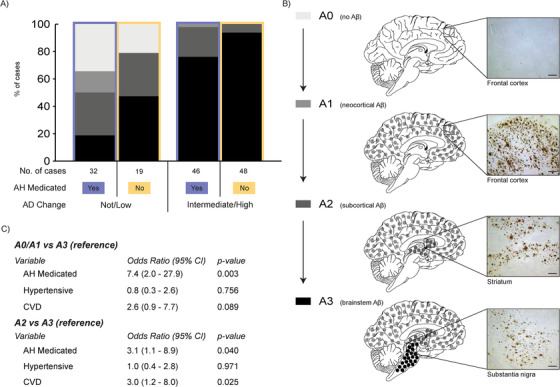
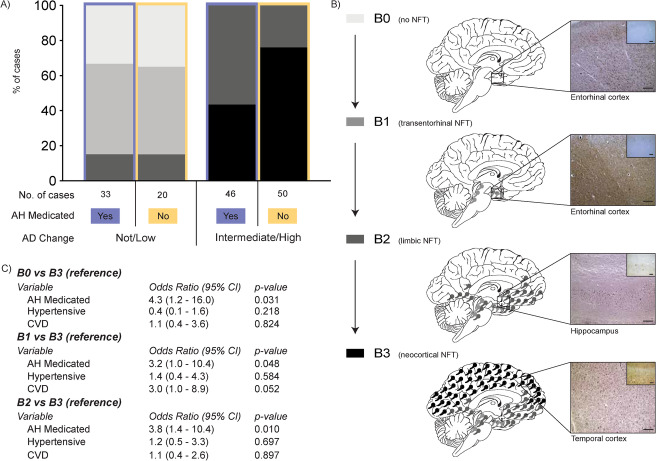
Results: Univariate analyses found no difference in amounts of AD proteins in the frontal cortex between medication users, but multivariate analyses showed that antihypertensive medication use was associated with a less extensive spread of AD proteins throughout the brain.
Discussion: The heterogeneous nature of the antihypertensive medications is consistent with downstream beneficial effects of blood pressure lowering and/or management being associated with the reduced spreading of AD pathology observed.
Keywords: Alzheimer's disease; amyloid; antihypertensive medication; neuropathology; tau.
© 2020 The Authors. Alzheimer's & Dementia: Translational Research & Clinical Interventions published by Wiley Periodicals LLC on behalf of Alzheimer's Association.
Conflict of interest statement
AA is a recipient of UNSW Brain Sciences Collaborative PhD Grant. PS is supported by research grants from the National Health & Medical Research Council, the Australian Research Council, the National Institute of Aging, the NHMRC National Institute for Dementia Research, and several philanthropic foundations. He reports no conflicts of interest in relation to this work. JS is funded by a research grant from the National Institute on Alcohol Abuse and Alcoholism of the National Institutes of Health (AA012725). GH consults for the National Health and Medical Research Council of Australia (NHMRC); received travel funds from AAIC, Int Soc Neurochemistry, Int DLB Conference, AAN, Int MSA Conference, NHMRC National Institute for Dementia Research, Japanese Neurology Soc; is on the editorial boards of Acta Neuropathol, J Neural Transm, J Parkinson Dis, Transl Neurodegen, Neuropathol Appl Neurobiol, receives royalties from Academic press, Elsevier & Oxford University Press; receives research grant funding from NHMRC, MJ Fox Foundation, Shake‐it‐up Australia, Parkinson's NSW, University of Sydney (infrastructure & equipment); and holds stock in Cochlear (2004 on) & NIB Holdings (2007 on).
Figures
References
-
- Azarpazhooh MR, Avan A, Cipriano LE, Munoz DG, Sposato LA, Hachinski V. Concomitant vascular and neurodegenerative pathologies double the risk of dementia. Alzheimers Dement. 2018;14:148‐156. - PubMed
-
- Lennon MJ, Makkar SR, Crawford JD, Sachdev PS. Midlife hypertension and alzheimer's disease: a systematic review and meta‐analysis. J Alzheimers Dis. 2019;71(1):307‐316. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources