

Association between periodontal disease and vulnerable plaque morphology in patients undergoing carotid endarterectomy
- PMID: 32802936
- PMCID: PMC7419330
- DOI: 10.1016/j.ijcha.2020.100601
Association between periodontal disease and vulnerable plaque morphology in patients undergoing carotid endarterectomy
Abstract
Background: Periodontal disease (PD) is a chronic inflammatory oral condition with potentially important systemic sequelae. We sought to determine whether the presence of PD in patients with severe carotid disease was associated with morphological features consistent with carotid plaque instability.
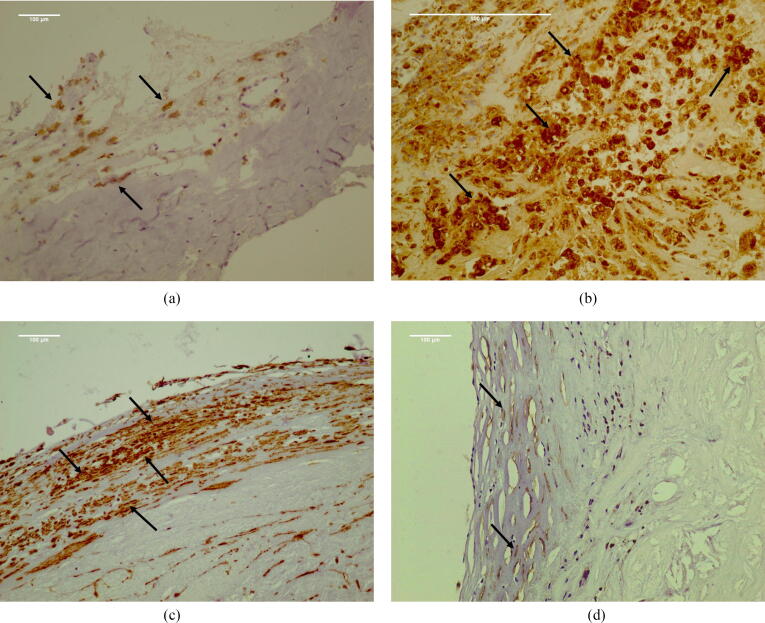
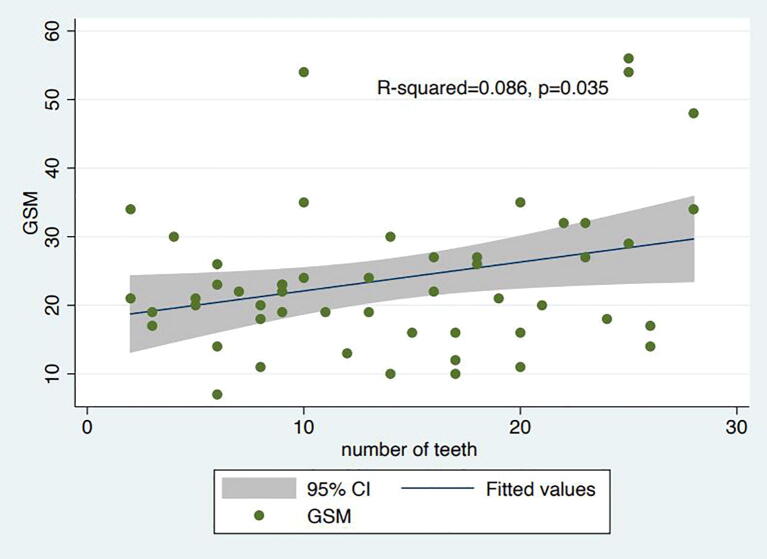
Methods: A total of 52 dentate patients hospitalized for carotid endarterectomy (CEA) had standardized assessments of their periodontal status, including measurements of probing pocket depth (PPD), clinical attachment level (CAL) and bleeding on probing (BoP). Carotid plaque morphology was assessed by ultrasound using the gray scale median (GSM) score and by immunohistochemistry using anti-CD68 and anti-alpha-actin antibodies, markers for macrophages and smooth muscle cells (SMCs) respectively.
Results: In total 30/52 patients (58%) had PD. Significant associations were noted between low GSM on ultrasound and each mm in PPD (p = 0.001), each mm in CAL (p = 0.002) and with a 10% increase in BoP (p = 0.009). Using the standardized PERIO definition the association remained robust (aOR = 10.4 [95% CI:2.3-46.3], p = .002). Significant associations were also observed with high macrophage accumulation and each individual PD measure (p < 0.01 for PPD, CAL and BoP) and with the PERIO definition (aOR = 15 [95% CI:1.8-127.8], p = .01). Similarly, low SMC density was also significantly associated with individual measures of PD (p < 0.05 for PPD, CAL and BoP), but not with the PERIO definition (aOR 3.4 [95% CI:0.9-12.8], p = .07).
Conclusions: The presence of PD was significantly associated with both ultrasound and immunohistochemistry features of carotid plaque instability in patients undergoing CEA.
Keywords: Carotid endarterectomy; Inflammation; Periodontal disease; Vulnerable plaque.
© 2020 Published by Elsevier B.V.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures




References
-
- Falk E., Shah P.K., Fuster V. Coronary plaque disruption. Circulation. 1995;92:657–671. - PubMed
-
- Yuan C., Kerwin W.S., Yarnykh V.L. MRI of atherosclerosis in clinical trials. NMR Biomed. 2006;19:636–654. - PubMed
-
- Biasi G.M., Froio A., Diethrich E.B. Carotid plaque echolucency increases the risk of stroke in carotid stenting: the Imaging in Carotid Angioplasty and Risk of Stroke (ICAROS) study. Circulation. 2004;110:756–762. - PubMed
-
- Papapanou P.N. Epidemiology of Periodontal diseases: an update. J. Int. Acad. Periodontol. 1999;1:110–116. - PubMed
LinkOut - more resources
Full Text Sources
