

Normocalcemic Hyperparathyroidism: A Heterogeneous Disorder Often Misdiagnosed?
- PMID: 32803112
- PMCID: PMC7422713
- DOI: 10.1002/jbm4.10391
Normocalcemic Hyperparathyroidism: A Heterogeneous Disorder Often Misdiagnosed?
Abstract
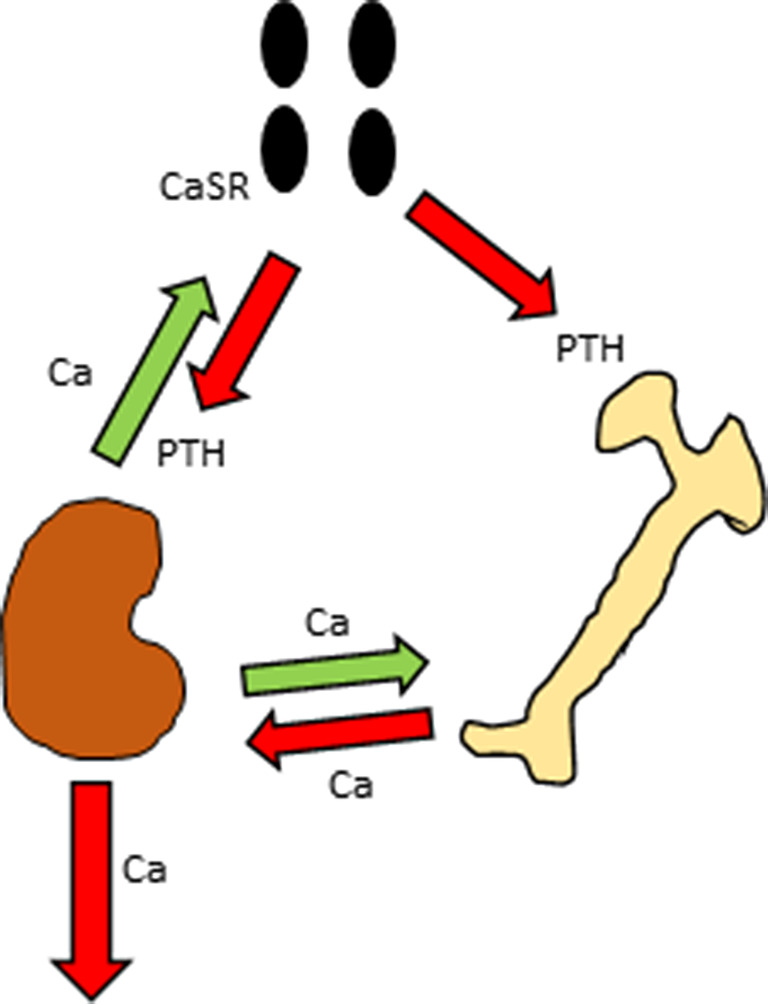
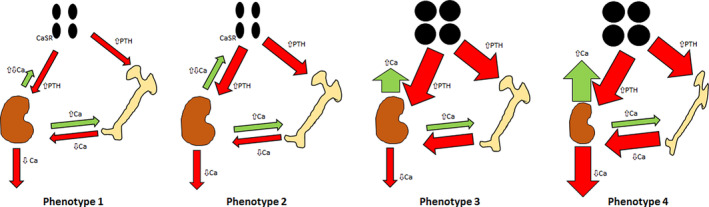
Normocalcemic primary hyperparathyroidism (NHPT) was first described over 10 years ago, but uncertainties still remain about its definition, prevalence, and rates of complications. As a result, consensus management guidelines for this condition have not yet been published. Several hypotheses have been proposed for the pathophysiology of NHPT, but it may be a heterogeneous disorder with multiple causes, rather than a single etiology that explains this biochemical phenotype. A common clinical concern is whether NHPT should be treated surgically when complications are already present at first recognition of the disorder, rather than following patients clinically over time. The literature on NHPT is based mostly on larger studies of population-based cohorts and smaller studies from referral centers. Lack of rigorous diagnostic criteria and selection bias inherent in populations seen at tertiary referral centers may explain the heterogeneity of reported rates of bone and renal complications in relation to consistently mild laboratory alterations. Unresolved questions remain about the significance of NHPT when it is diagnosed biochemically without evident bone or kidney complications. Moreover, its natural history remains to be elucidated because a proportion of what is classified as NHPT may revert to normal spontaneously, thus revealing previously unrecognized secondary hyperparathyroidism. These issues indicate that caution should be used in recommending surgery for NHPT. This review will focus on recent issues regarding the pathophysiology, evaluation, and management of NHPT. © 2020 The Authors. JBMR Plus published by Wiley Periodicals LLC on behalf of American Society for Bone and Mineral Research.
Keywords: HYPERCALCEMIA; HYPERCALCIURIA; NEPHROLITHIASIS; NORMOCALCEMIC HYPERPARATHYROIDISM; OSTEOPOROSIS; PRIMARY HYPERPARATHYROIDISM; SECONDARY HYPERPARATHYROIDISM.
© 2020 The Authors. JBMR Plus published by Wiley Periodicals LLC on behalf of American Society for Bone and Mineral Research.
Figures
References
-
- Clarke BL. Asymptomatic primary hyperparathyroidism. Front Horm Res. 2018;51:13–22. - PubMed
-
- Cusano NE, Cipriani C, Bilezikian JP. Management of normocalcemic primary hyperparathyroidism. Best Pract Res Clin Endocrinol Metab. 2018;32(6):837–45. - PubMed
-
- Eastell R, Brandi ML, Costa AG, D'Amour P, Shoback DM, Thakker RV. Diagnosis of asymptomatic primary hyperparathyroidism: proceedings of the fourth international workshop. J Clin Endocrinol Metab. 2014;99(10):3570–9. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials