

Invasive Group A Streptococcal Infections Among People Who Inject Drugs and People Experiencing Homelessness in the United States, 2010-2017
- PMID: 32803254
- PMCID: PMC8938854
- DOI: 10.1093/cid/ciaa787
Invasive Group A Streptococcal Infections Among People Who Inject Drugs and People Experiencing Homelessness in the United States, 2010-2017
Abstract
Background: Reported outbreaks of invasive group A Streptococcus (iGAS) infections among people who inject drugs (PWID) and people experiencing homelessness (PEH) have increased, concurrent with rising US iGAS rates. We describe epidemiology among iGAS patients with these risk factors.
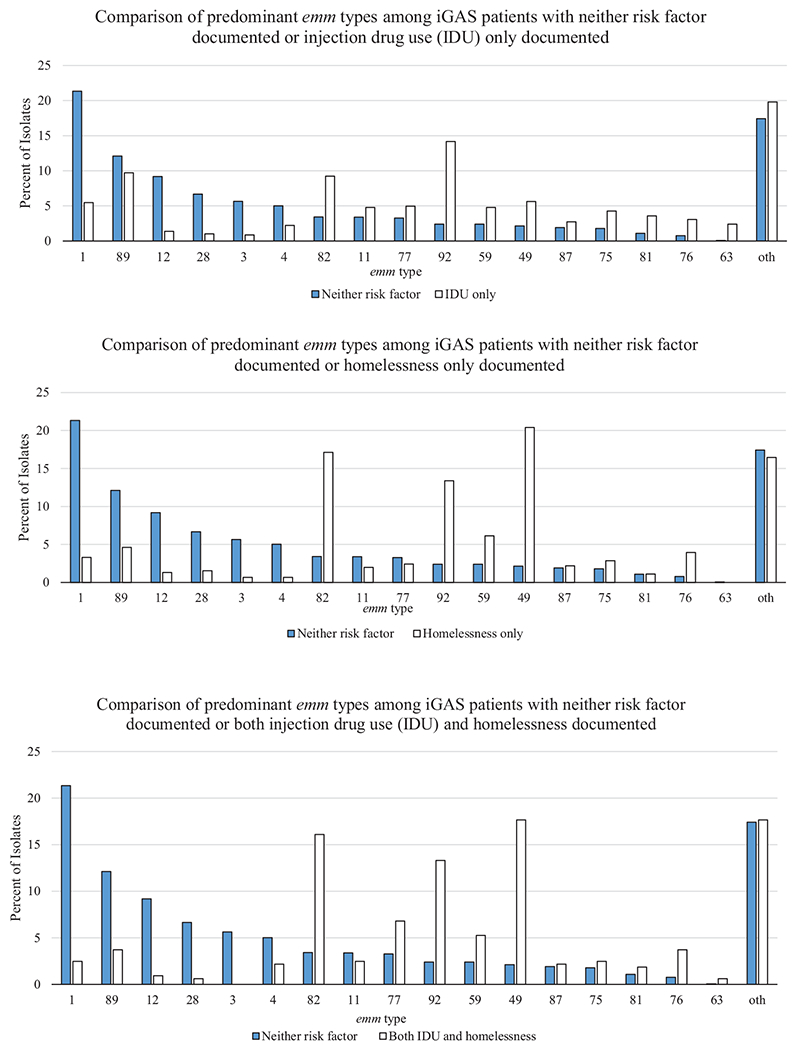
Methods: We analyzed iGAS infections from population-based Active Bacterial Core surveillance (ABCs) at 10 US sites from 2010 to 2017. Cases were defined as GAS isolated from a normally sterile site or from a wound in patients with necrotizing fasciitis or streptococcal toxic shock syndrome. GAS isolates were emm typed. We categorized iGAS patients into four categories: injection drug use (IDU) only, homelessness only, both, and neither. We calculated annual change in prevalence of these risk factors using log binomial regression models. We estimated national iGAS infection rates among PWID and PEH.
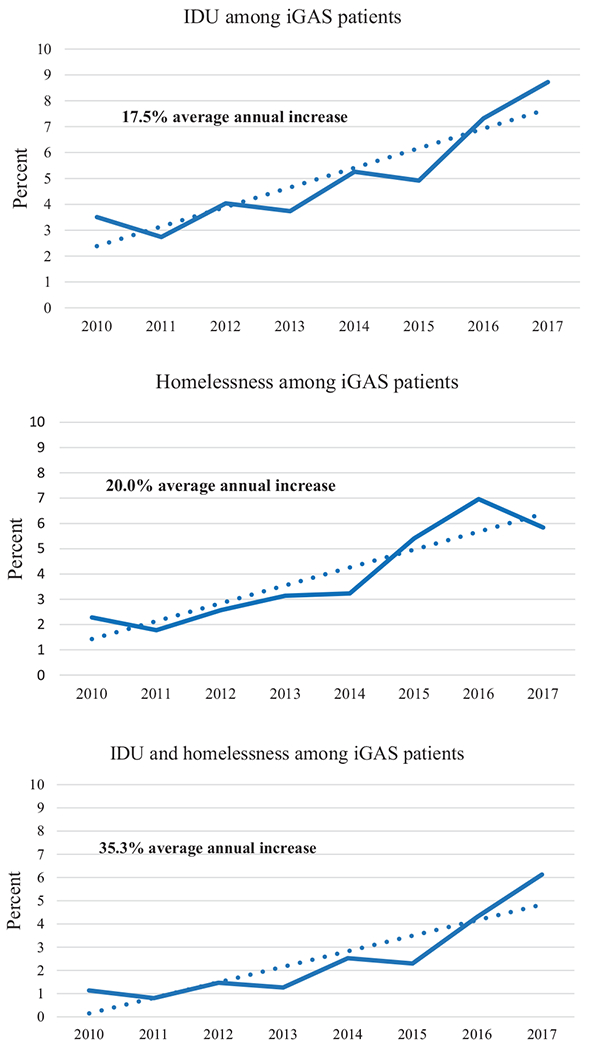
Results: We identified 12 386 iGAS cases; IDU, homelessness, or both were documented in ~13%. Skin infections and acute skin breakdown were common among iGAS patients with documented IDU or homelessness. Endocarditis was 10-fold more frequent among iGAS patients with documented IDU only versus those with neither risk factor. Average percentage yearly increase in prevalence of IDU and homelessness among iGAS patients was 17.5% and 20.0%, respectively. iGAS infection rates among people with documented IDU or homelessness were ~14-fold and 17- to 80-fold higher, respectively, than among people without those risks.
Conclusions: IDU and homelessness likely contribute to increases in US incidence of iGAS infections. Improving management of skin breakdown and early recognition of skin infection could prevent iGAS infections in these patients.
Keywords: epidemiology; group A Streptococcus; homelessness; injection drug use; surveillance.
Published by Oxford University Press for the Infectious Diseases Society of America 2020.
Conflict of interest statement
Figures
References
-
- Centers for Disease Control and Prevention. Active Bacterial Core surveillance (ABCs) report, Emerging Infections Program Network, group A Streptococcus, 2010. Available at: https://www.cdc.gov/abcs/reports-findings/survreports/gas10.pdf. Accessed 29 April 2020.
-
- Centers for Disease Control and Prevention. Active Bacterial Core surveillance (ABCs) report, Emerging Infections Program Network, group A Streptococcus, 2017. Available at https://www.cdc.gov/abcs/reports-findings/survreports/gas17.pdf. Accessed 29 April 2020.
-
- Jordan HT, Richards CL Jr, Burton DC, Thigpen MC, Van Beneden CA. Group A streptococcal disease in long-term care facilities: descriptive epidemiology and potential control measures. Clin Infect Dis 2007; 45:742–52. - PubMed
-
- Dooling KL, Crist MB, Nguyen DB, et al. Investigation of a prolonged group A streptococcal outbreak among residents of a skilled nursing facility, Georgia, 2009–2012. Clin Infect Dis 2013; 57:1562–7. - PubMed
-
- Deutscher M, Schillie S, Gould C, et al. Investigation of a group A streptococcal outbreak among residents of a long-term acute care hospital. Clin Infect Dis 2011; 52:988–94. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
