

Large airway-obstructing retropharyngeal lipoma in an asymptomatic patient: a case report
- PMID: 32803431
- PMCID: PMC7429597
- DOI: 10.1186/s40729-020-00237-3
Large airway-obstructing retropharyngeal lipoma in an asymptomatic patient: a case report
Abstract
Background: Lipomas are common benign mesenchymal tumors that appear in the head and neck region in approximately 25% of cases where they are noted. Lipomas of the airway region are exceedingly rare, accounting for less than 1% of airway obstruction tumors. Correlation of radiographic findings from cone beam computed tomography (CBCT), multi-detector computed tomography (MDCT), and magnetic resonance imaging (MRI) of a rare retropharyngeal lipoma has not been previously reported. CBCT studies acquired for implant and/or other diagnostic purposes may be the first line of detection as an incidental finding.
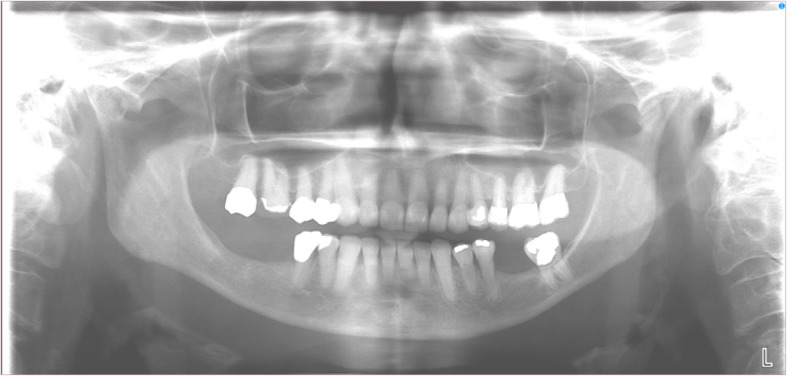
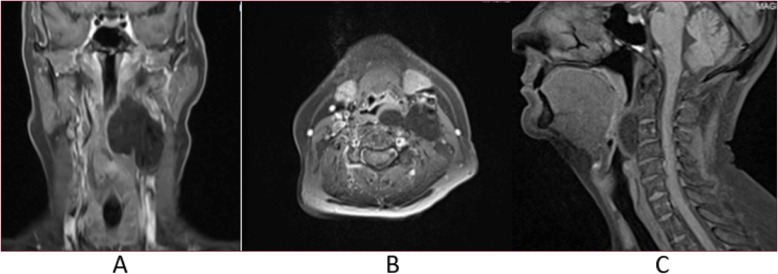
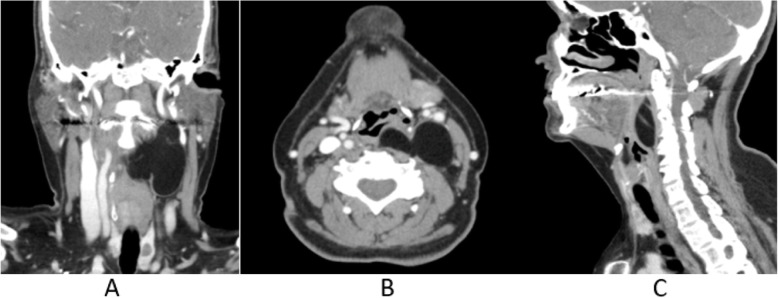
Case presentation: A 66-year-old female presented for a pre-implant CBCT with no history of other complaints or signs/symptoms. CBCT imaging depicts a large, well-defined, low-attenuation/soft tissue density lesion with an undulating appearance extending from the posterior left pharyngeal wall and occluding two-thirds of the airway from C2 to C4. The lesion extends laterally into the left parapharyngeal space and inferiorly beyond the field of view of the study. Evidence of faint internal septations was noted. The patient was immediately referred for an ENT consult. Laryngoscopy, MRI, and contrast-enhanced MDCT imaging were conducted to determine the full extent and nature of the lesion, as well as to potentially plan for biopsy and/or surgical resection. Removal of the lesion was successful, and histopathologic evaluation confirmed lipoma. Periodic follow-up was recommended to monitor for possible recurrence.
Discussion: The slower growth pattern of some benign lesions may obscure any symptoms as changes the patient may normally notice take place over an extended period. Furthermore, soft tissue lesions and especially those in the posterior midline, such as in this case, may not be easily visible on routine panoramic imaging or clinical exam, allowing for substantially large growth before detection. While the soft tissue contrast of the CBCT volume is poor, enough information was present to establish an initial differential diagnosis and the need for more advanced imaging modalities. With the growing popularity and adoption of CBCT in maxillofacial imaging, a thorough understanding of the appearance of hard and soft tissue lesions, as well as a strong understanding of the baseline appearance of normal anatomy, is important to ensure no incidental pathoses go undiagnosed.
Keywords: CBCT; Lipoma; MDCT; MRI; OMFR; Retropharyngeal.
Conflict of interest statement
Scott A. Ehlers, John M. Bozanich, Mehrnaz Tahmasbi Arashlow, Hui Liang, and Madhu K Nair declare that they have no competing interests.
Figures


References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
