

Pre- and post-operative imaging of cochlear implants: a pictorial review
- PMID: 32803542
- PMCID: PMC7429612
- DOI: 10.1186/s13244-020-00902-6
Pre- and post-operative imaging of cochlear implants: a pictorial review
Abstract
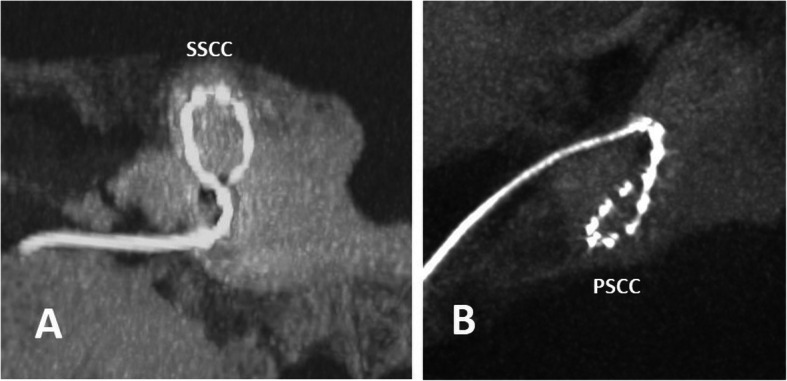
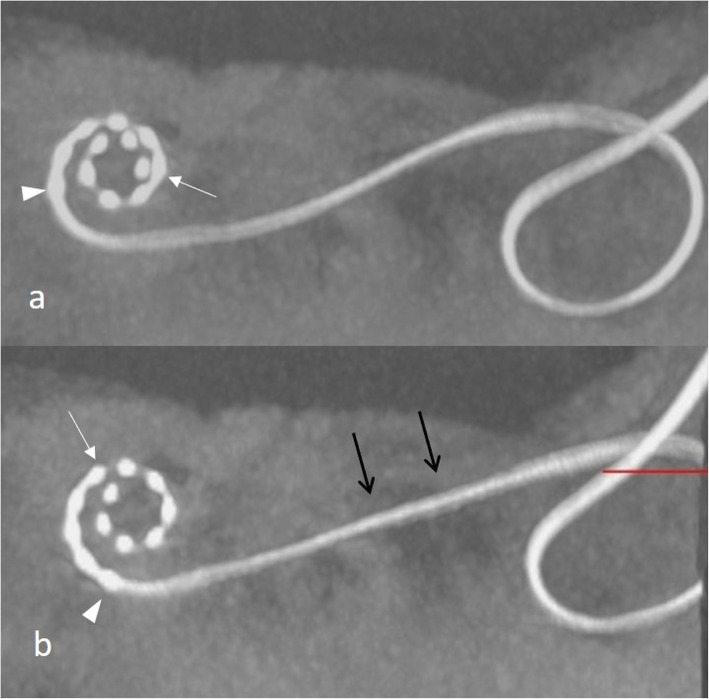
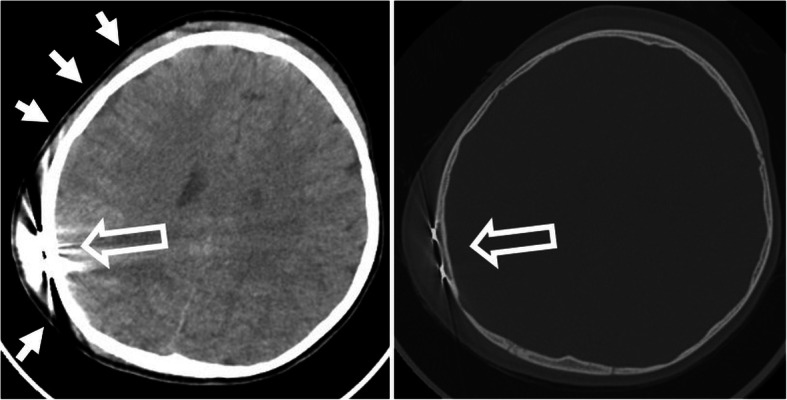
Cochlear implants are increasingly used to treat sensorineural hearing disorders in both children and adults. Pre-operative computed tomography and magnetic resonance imaging play a pivotal role in patient selection, to rule out findings that preclude surgery or identify conditions which may have an impact on the surgical procedure. The post-operative position of the electrode array within the cochlea can be reliably identified using cone-beam computed tomography. Recognition of scalar dislocation, cochlear dislocation, electrode fold, and malposition of the electrode array may have important consequences for the patient such as revision surgery or adapted fitting.
Keywords: Cochlear implant; Electrode array position; Post-operative imaging; Pre-operative imaging.
Conflict of interest statement
JS has an active scientific grant with the MedEL Company.
All other authors declare that they do not have any competing interests related to this article.
Figures
References
-
- Carlson ML, Sladen DP, Gurgel RK, Tombers NM, Lohse CM, Driscoll CL. Survey of the American Neurotology Society on cochlear implantation: part 1, candidacy assessment and expanding indications. Otol Neurotol. 2018;39:e12–e19. - PubMed
-
- Vesseur A, Free R, Snels C, et al. Hearing restoration in cochlear nerve deficiency: the choice between cochlear implant or auditory brainstem implant, a meta-analysis. Otol Neurotol. 2018;39:428–437. - PubMed
-
- Peng KA, Kuan EC, Hagan S, Wilkinson EP, Miller ME. Cochlear nerve aplasia and hypoplasia: predictors of cochlear implant success. Otolaryngol Head Neck Surg. 2017;157:392–400. - PubMed
-
- Birman CS, Brew JA, Gibson WPR, Elliott EJ. CHARGE syndrome and cochlear implantation: difficulties and outcomes in the paediatric population. Int J Pediatr Otorhinolaryngol. 2015;79:487–492. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
