

Management of Thrombotic Complications in COVID-19: An Update
- PMID: 32803670
- PMCID: PMC7429134
- DOI: 10.1007/s40265-020-01377-x
Management of Thrombotic Complications in COVID-19: An Update
Abstract
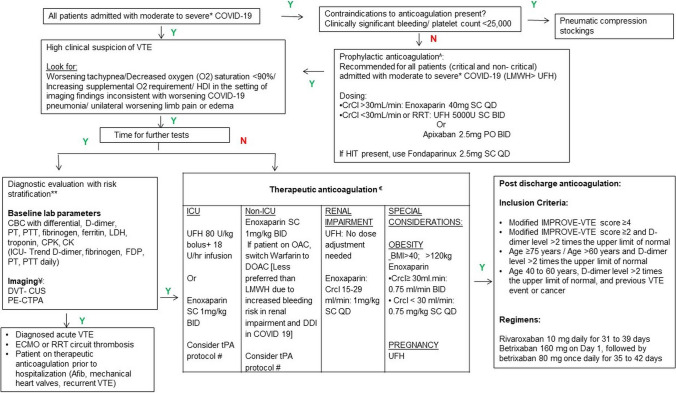
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV‑2), is now a global pandemic. This virus primarily affects the respiratory tract and causes lung injury characterized by acute respiratory distress syndrome. Although the pathophysiology of COVID-19 is not yet clear, the most widely accepted mechanism is systemic inflammation. A clinically significant effect of the inflammation is coagulopathy. As a result of this effect, patients are found to have a high risk of venous thromboembolism. Studies have reported a high incidence of thrombotic complications in critically ill patients with COVID-19. In this review, we discuss the most updated evidence on the pathophysiology, diagnosis, and treatment of the coagulopathy of COVID-19. Prophylactic anticoagulation is recommended for all in-patients with COVID-19. Those with a higher risk of developing thromboembolic events or who have already developed venous thromboembolism should be treated with therapeutic anticoagulation. We also discuss post-discharge prophylaxis for high-risk patients and some newly proposed treatments for the hypercoagulability that could improve the outcomes of the affected patients.
Conflict of interest statement
Adrija Hajra, Sheetal Vasundara Mathai, Somedeb Ball, Dhrubajyoti Bandyopadhyay, Maedeh Veyseh, Sandipan Chakraborty, Carl J. Lavie, and Wilbert S. Aronow have no conflicts of interest that are directly relevant to the content of this article.
Figures
References
-
- Center for Disease Control (CDC). Cases in the US. Available from: https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html. Accessed 10 June 2020.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
