

Developing a cognitive behavioral therapy for hypersomnia using telehealth: a feasibility study
- PMID: 32804069
- PMCID: PMC7848927
- DOI: 10.5664/jcsm.8750
Developing a cognitive behavioral therapy for hypersomnia using telehealth: a feasibility study
Abstract
Study objectives: The purpose of this study was to evaluate the feasibility and acceptability of a novel cognitive behavioral therapy for hypersomnia (CBT-H) in people with central disorders of hypersomnolence and co-occurring depressive symptoms using a telehealth model for delivery and assessment.
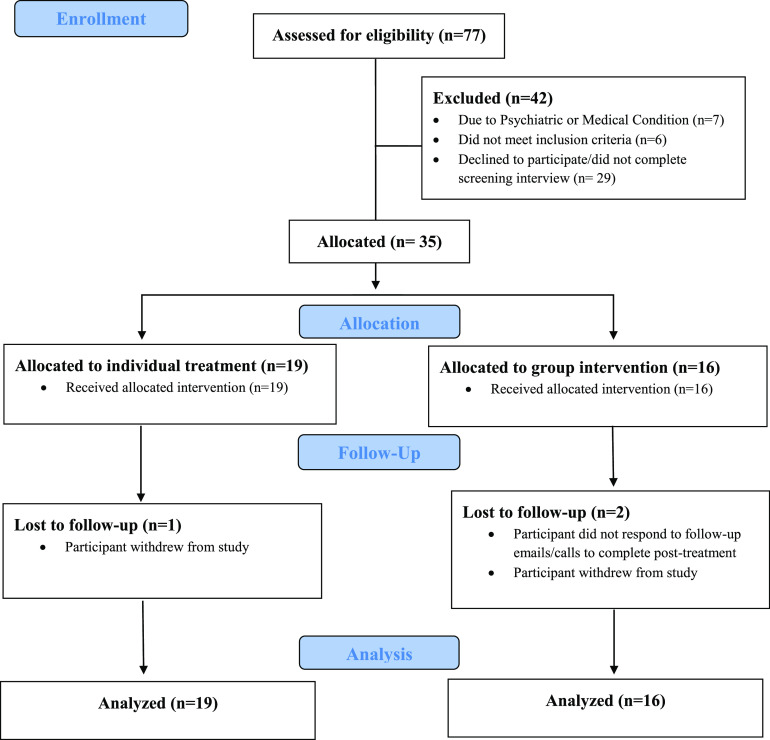
Methods: Thirty-five adults with narcolepsy or idiopathic hypersomnia received a 6-session CBT-H delivered individually or in small groups using videoconferencing. The clinical impact of CBT-H was evaluated using the Patient Health Questionnaire, Patient-Reported Outcomes Measurement Information System measures, Epworth Sleepiness Scale, and other patient-reported outcomes collected online at baseline and posttreatment. Feasibility and acceptability of the intervention and telehealth model was also evaluated using qualitative data collected from exit interviews conducted through videoconferencing.
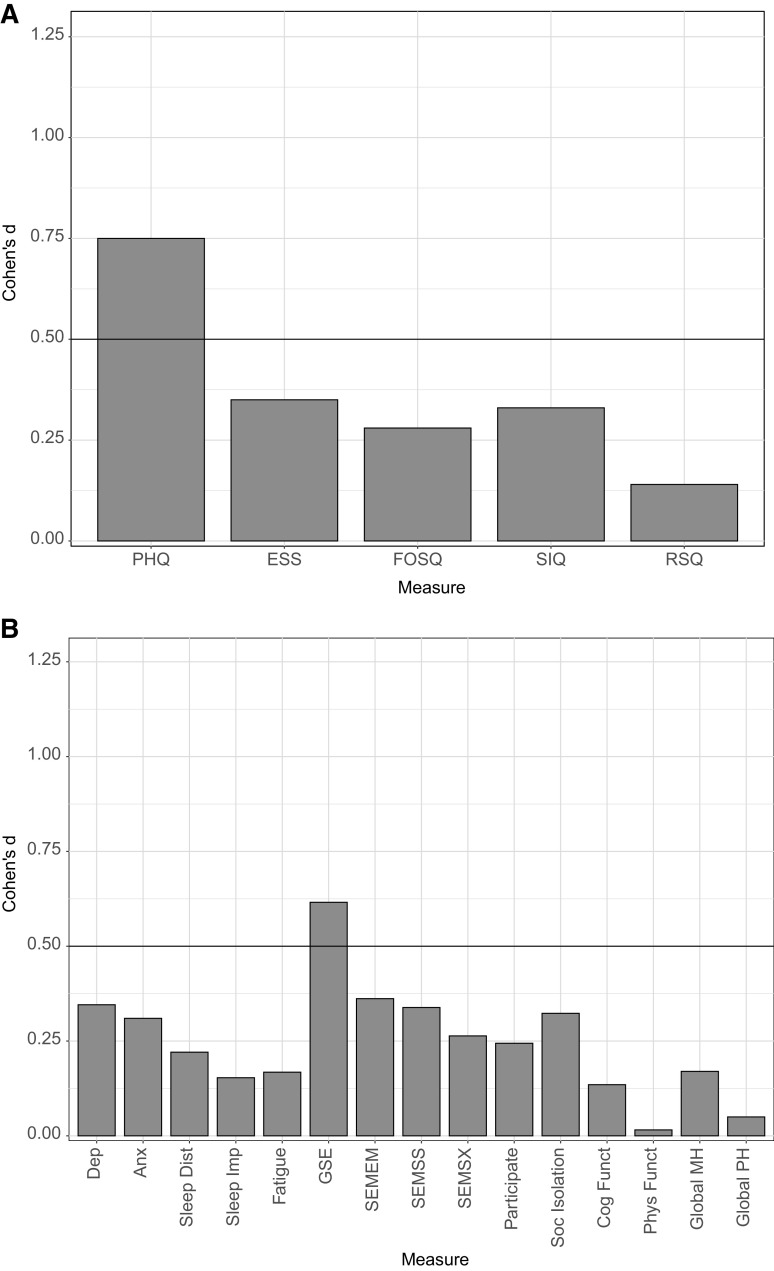
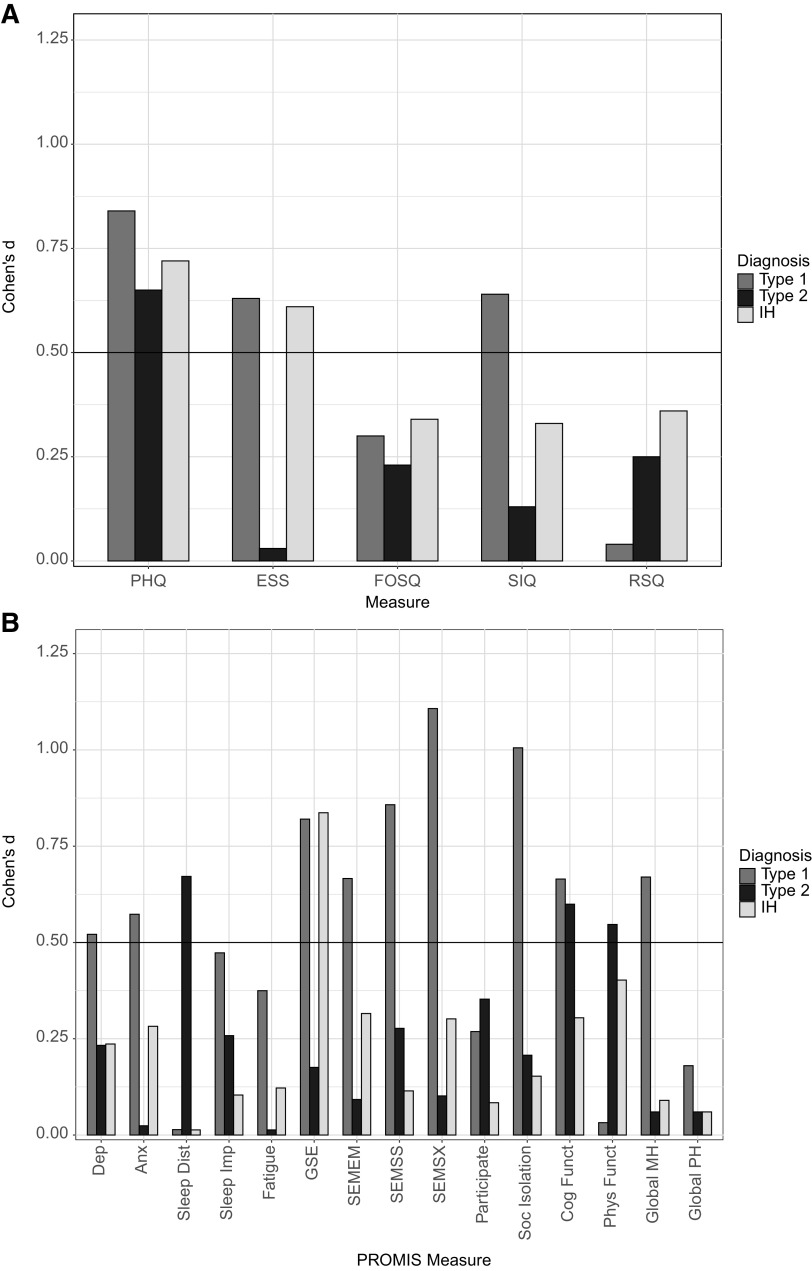
Results: Forty percent of the sample achieved a clinically significant baseline to posttreatment change in depressive symptoms (decrease in Patient Health Questionnaire ≥ 5), which is below the prespecified efficacy benchmark (50% of the sample). The prespecified benchmark for a minimal clinically important difference (Cohen's d > 0.5) on other psychosocial measures was met only on the Patient-Reported Outcomes Measurement Information System global self-efficacy (d = 0.62) in the total sample. Qualitative data revealed enthusiasm for the accessibility of telehealth delivery and the usefulness of several cognitive and behavioral modules but also revealed opportunities to refine the CBT-H program.
Conclusions: These findings indicate that this new CBT-H program can potentially reduce depressive symptoms and improve self-efficacy in people with central disorders of hypersomnolence. Furthermore, telehealth is a promising model for remote delivery and data collection to enhance participant accessibility and engagement.
Clinical trial registration: Registry: ClinicalTrials.gov; Name: Psychosocial Adjunctive Treatment for Hypersomnia (PATH); URL: https://clinicaltrials.gov/ct2/show/NCT03904238; Identifier: NCT03904238.
Keywords: cognitive-behavior therapy; depression; health-related quality of life; idiopathic hypersomnia; narcolepsy; psychosocial.
© 2020 American Academy of Sleep Medicine.
Figures
References
-
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Association; 2013.
-
- Ozaki A, Inoue Y, Nakajima T, Hayashida K, Honda M, Komada Y, Takahashi K. Health-related quality of life among drug-naïve patients with narcolepsy with cataplexy, narcolepsy without cataplexy, and idiopathic hypersomnia without long sleep time. J Clin Sleep Med. 2008;4(6):572–578. 10.5664/jcsm.27352 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
