

International Survey to Establish Prioritized Outcomes for Trials in People With Coronavirus Disease 2019
- PMID: 32804789
- PMCID: PMC7448718
- DOI: 10.1097/CCM.0000000000004584
International Survey to Establish Prioritized Outcomes for Trials in People With Coronavirus Disease 2019
Abstract
Objectives: There are over 4,000 trials conducted in people with coronavirus disease 2019. However, the variability of outcomes and the omission of patient-centered outcomes may diminish the impact of these trials on decision-making. The aim of this study was to generate a consensus-based, prioritized list of outcomes for coronavirus disease 2019 trials.
Design: In an online survey conducted in English, Chinese, Italian, Portuguese, and Spanish languages, adults with coronavirus disease 2019, their family members, health professionals, and the general public rated the importance of outcomes using a 9-point Likert scale (7-9, critical importance) and completed a Best-Worst Scale to estimate relative importance. Participant comments were analyzed thematically.
Setting: International.
Subjects: Adults 18 years old and over with confirmed or suspected coronavirus disease 2019, their family members, members of the general public, and health professionals (including clinicians, policy makers, regulators, funders, and researchers).
Interventions: None.
Measurements: None.
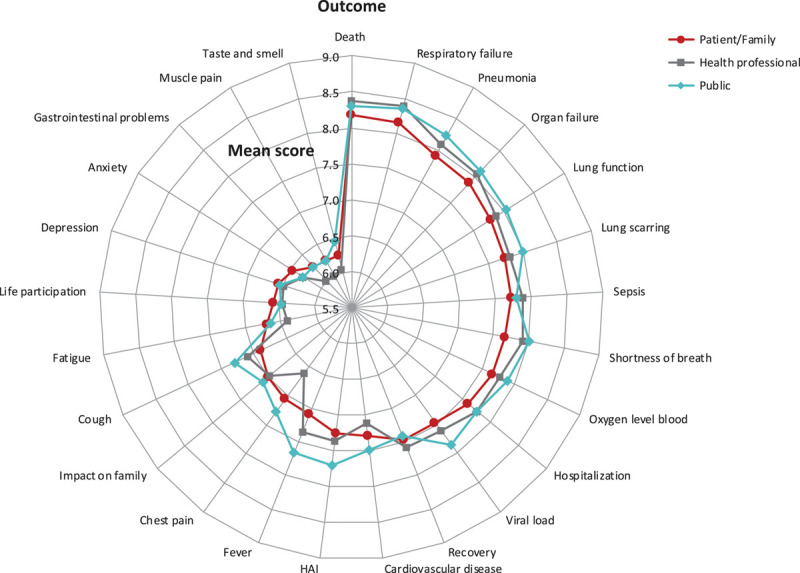
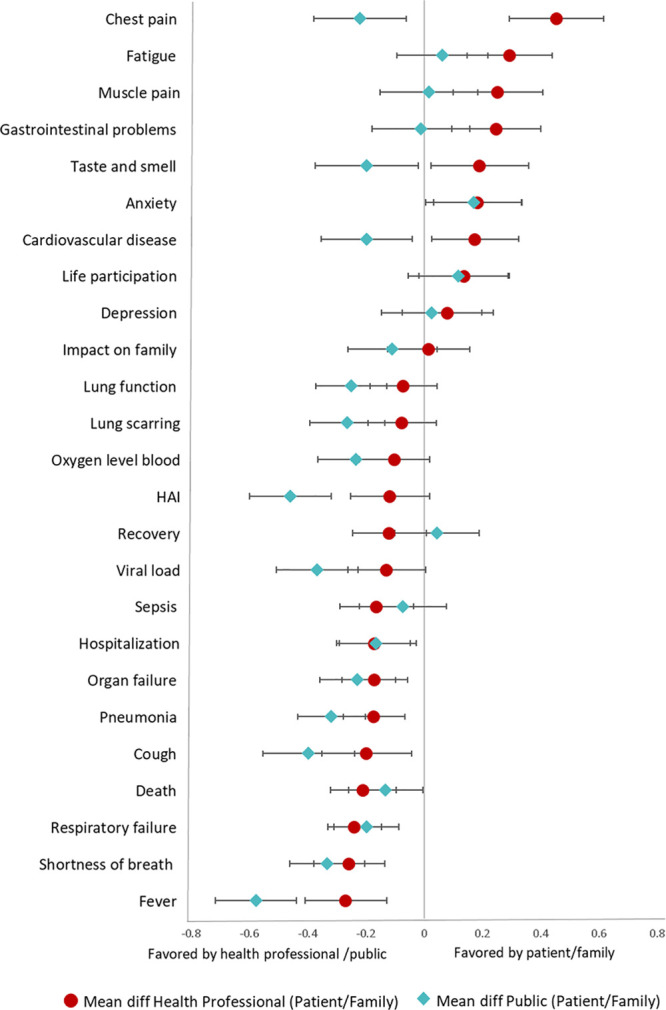
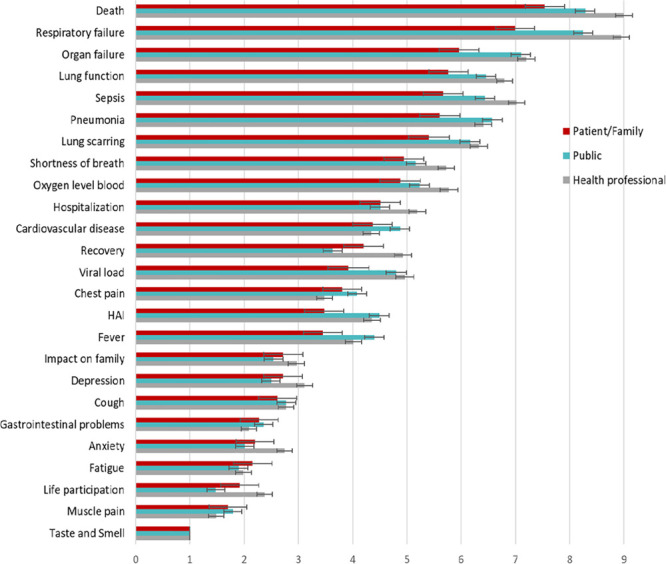
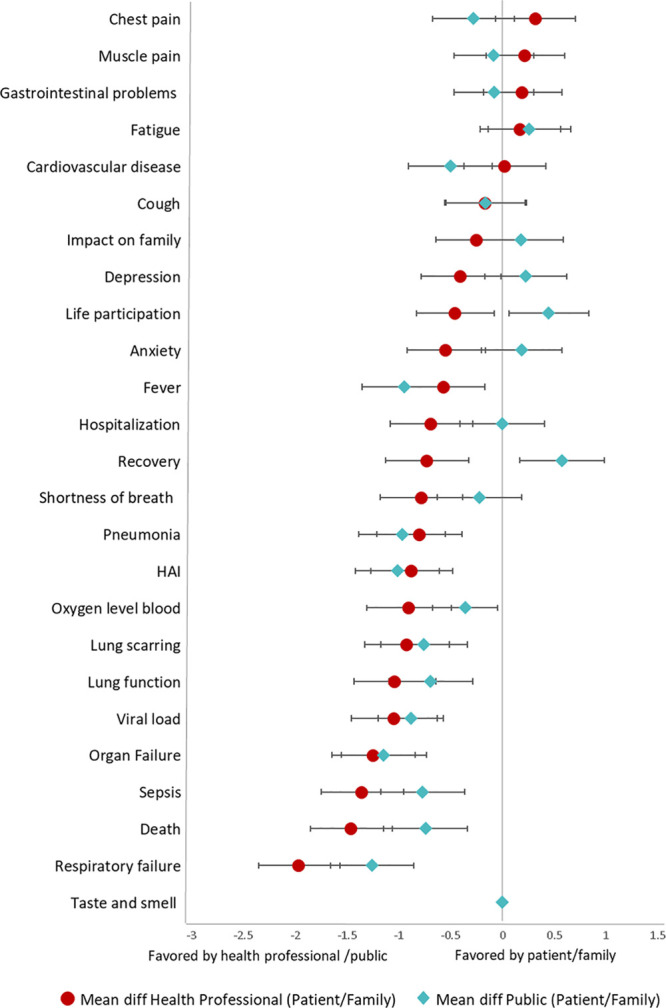
Main results: In total, 9,289 participants from 111 countries (776 people with coronavirus disease 2019 or family members, 4,882 health professionals, and 3,631 members of the public) completed the survey. The four outcomes of highest priority for all three groups were: mortality, respiratory failure, pneumonia, and organ failure. Lung function, lung scarring, sepsis, shortness of breath, and oxygen level in the blood were common to the top 10 outcomes across all three groups (mean > 7.5, median ≥ 8, and > 70% of respondents rated the outcome as critically important). Patients/family members rated fatigue, anxiety, chest pain, muscle pain, gastrointestinal problems, and cardiovascular disease higher than health professionals. Four themes underpinned prioritization: fear of life-threatening, debilitating, and permanent consequences; addressing knowledge gaps; enabling preparedness and planning; and tolerable or infrequent outcomes.
Conclusions: Life-threatening respiratory and other organ outcomes were consistently highly prioritized by all stakeholder groups. Patients/family members gave higher priority to many patient-reported outcomes compared with health professionals.
Conflict of interest statement
Dr. Tong is supported by The University of Sydney Robinson Fellowship. Dr. Morris is supported by a Clinical Research Career Development Fellowship from the Wellcome Trust (WT 2055214/Z/16/Z). Dr. Douglas is principal investigator of clinical and translational research studies of acute respiratory distress syndrome, sepsis, and coronavirus disease 2019 from National Institutes of Health, Roche Pharmaceuticals, and Genentech. Research grants are to his institution, Denver Health Medical Center. Dr. Povoa had received lecture fees from Orion, Pfizer, and Technofage. Dr. Azevedo received funding from Pfizer and Halex-Istar. Dr. Mer received funding from Pfizer, MSD, Sanofi Aventis, Aspen, and Astellas. Dr. Morris received support for article research from Wellcome Trust/COAF. Dr. Smyth's institution received funding from Vertex; he received funding from Vertex, Teva, and Novartis; and he has a patent issued “Alkyl quinolones as biomarkers of Pseudomonas aeruginosa infection and uses thereof.” Dr. Turner's institution received funding from Stroke Foundation, Australian Medical Research Future Fund, Victorian State Government, and she disclosed that she is employed by Monash University; provides technical advice to WHO and Australian Red Cross Lifeblood; has undertaken consultancies for USAID, the Burnet Institute, and WHO; works on a shared MRFF research grant with the Stroke Foundation, and conducts research funded by Australian Commonwealth and State research funding agencies. Dr. Cho's institution received funding from Baxter and project grants through the NHMRC and HRC of New Zealand; he received funding from Baxter; he receives stipend from the Peritoneal Dialysis International (Associate Editor); and he is the current recipient of the National Health and Medical Research Council early career fellowship awarded by the Australian government. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- World Health Organization: Coronavirus Disease (Covid-19) Pandemic. 2020. Available at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019. Accessed April 27, 2020
MeSH terms
LinkOut - more resources
Full Text Sources
