

Timing of Intubation and Mortality Among Critically Ill Coronavirus Disease 2019 Patients: A Single-Center Cohort Study
- PMID: 32804790
- PMCID: PMC7448713
- DOI: 10.1097/CCM.0000000000004600
Timing of Intubation and Mortality Among Critically Ill Coronavirus Disease 2019 Patients: A Single-Center Cohort Study
Abstract
Objectives: Increasing time to mechanical ventilation and high-flow nasal cannula use may be associated with mortality in coronavirus disease 2019. We examined the impact of time to intubation and use of high-flow nasal cannula on clinical outcomes in patients with coronavirus disease 2019.
Design: Retrospective cohort study.
Setting: Six coronavirus disease 2019-specific ICUs across four university-affiliated hospitals in Atlanta, Georgia.
Patients: Adults with laboratory-confirmed severe acute respiratory syndrome coronavirus 2 infection who received high-flow nasal cannula or mechanical ventilation.
Interventions: None.
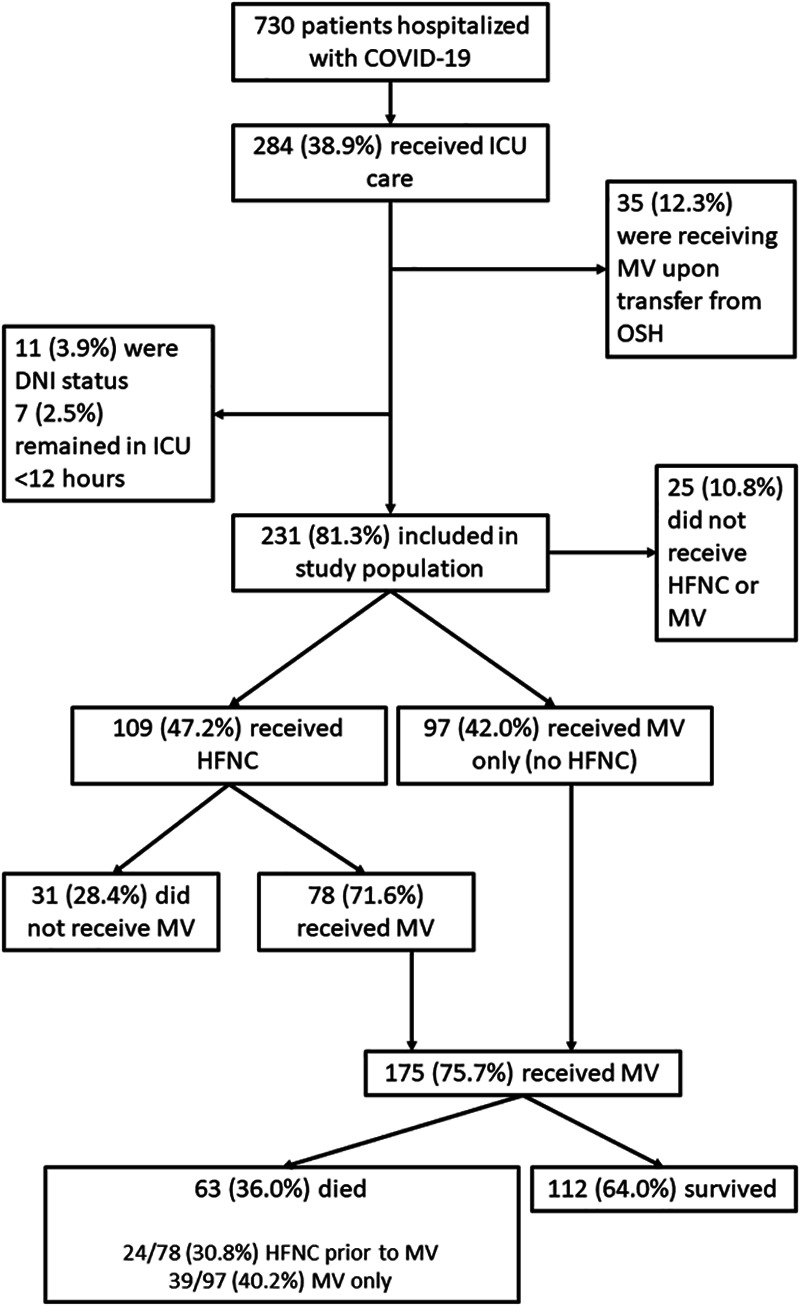
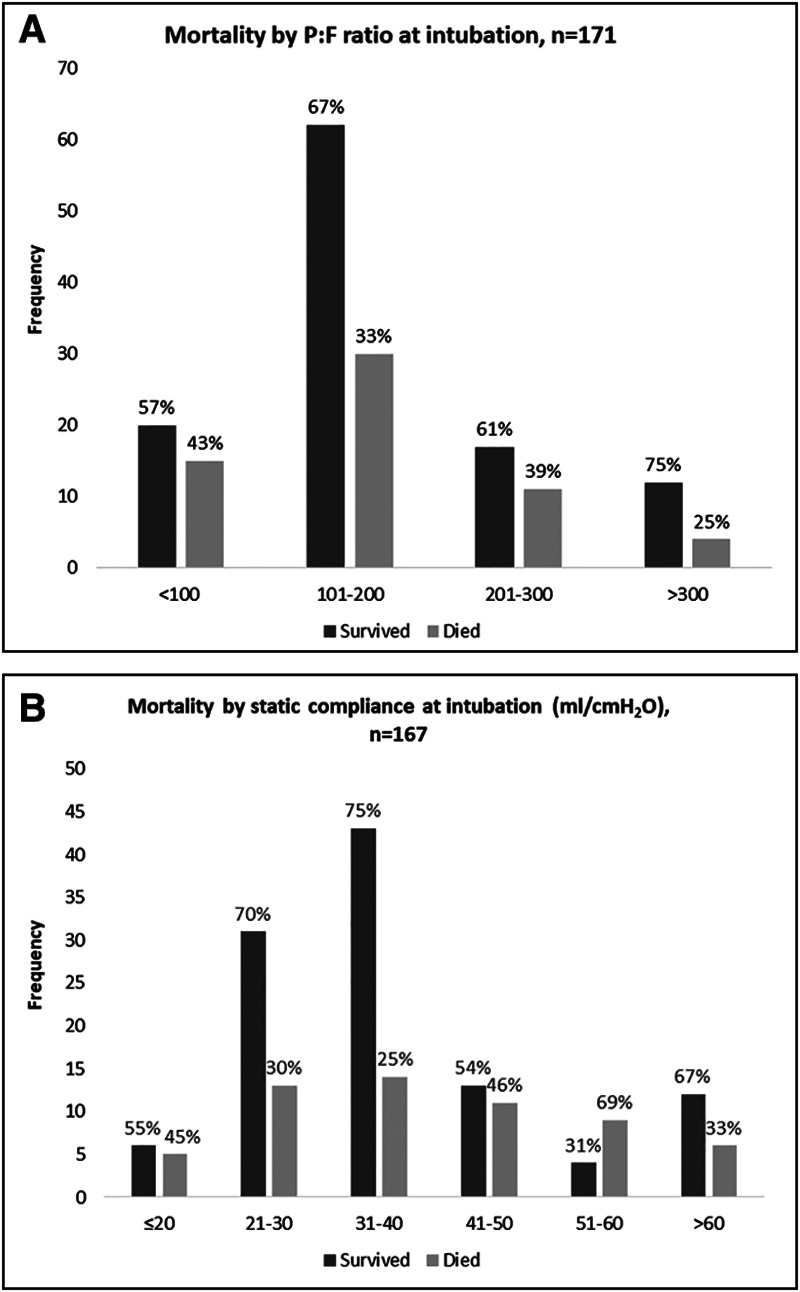
Measurements and main results: Among 231 patients admitted to the ICU, 109 (47.2%) were treated with high-flow nasal cannula and 97 (42.0%) were intubated without preceding high-flow nasal cannula use. Of those managed with high-flow nasal cannula, 78 (71.6%) ultimately received mechanical ventilation. In total, 175 patients received mechanical ventilation; 44.6% were female, 66.3% were Black, and the median age was 66 years (interquartile range, 56-75 yr). Seventy-six patients (43.4%) were intubated within 8 hours of ICU admission, 57 (32.6%) between 8 and 24 hours of admission, and 42 (24.0%) greater than or equal to 24 hours after admission. Patients intubated within 8 hours were more likely to have diabetes, chronic comorbidities, and higher admission Sequential Organ Failure Assessment scores. Mortality did not differ by time to intubation (≤ 8 hr: 38.2%; 8-24 hr: 31.6%; ≥ 24 hr: 38.1%; p = 0.7), and there was no association between time to intubation and mortality in adjusted analysis. Similarly, there was no difference in initial static compliance, duration of mechanical ventilation, or ICU length of stay by timing of intubation. High-flow nasal cannula use prior to intubation was not associated with mortality.
Conclusions: In this cohort of critically ill patients with coronavirus disease 2019, neither time from ICU admission to intubation nor high-flow nasal cannula use were associated with increased mortality. This study provides evidence that coronavirus disease 2019 respiratory failure can be managed similarly to hypoxic respiratory failure of other etiologies.
Conflict of interest statement
Dr. Blum’s institution received funding from the National Institutes of Health (NIH), and he received funding from Clew Medical. Drs. Blum and Auld received support for article research from the NIH. Dr. Martin disclosed he currently serves as president-elect for the Society of Critical Care Medicine. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
