

Comparison of World Health Organization and Demographic and Health Surveys data to estimate sub-national deworming coverage in pre-school aged children
- PMID: 32804925
- PMCID: PMC7462292
- DOI: 10.1371/journal.pntd.0008551
Comparison of World Health Organization and Demographic and Health Surveys data to estimate sub-national deworming coverage in pre-school aged children
Abstract
Background: The key metric for monitoring the progress of deworming programs in controlling soil-transmitted helminthiasis (STH) is national drug coverage reported to the World Health Organization (WHO). There is increased interest in utilizing geographically-disaggregated data to estimate sub-national deworming coverage and equity, as well as gender parity. The Demographic and Health Surveys (DHS) offer a potential source of sub-national data. This study aimed to compare deworming coverage routinely reported to WHO and estimated by DHS in pre-school aged children to inform global STH measurement and evaluation.
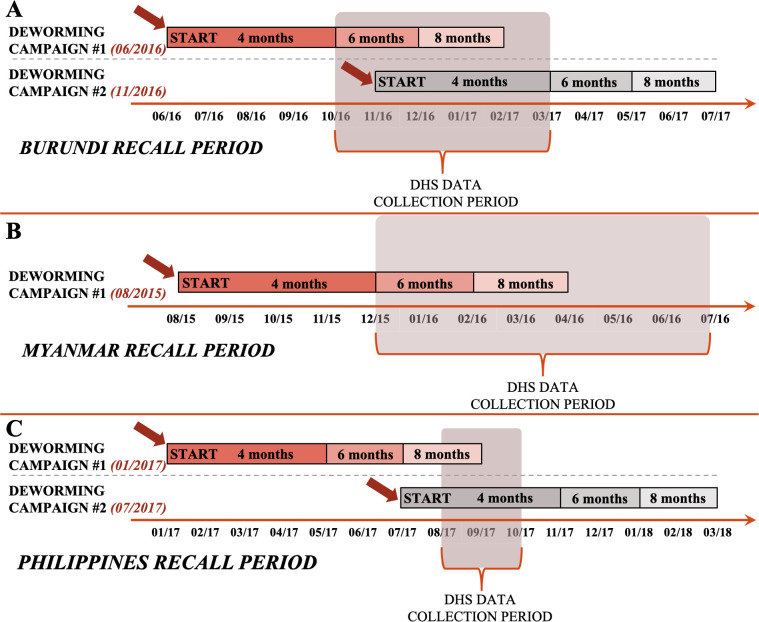
Methodology: We compared sub-national deworming coverage in pre-school aged children reported to WHO and estimated by DHS aligned geospatially and temporally. We included data from Burundi (2016-2017), Myanmar (2015-2016), and the Philippines (2017) based on data availability. WHO provided data on the date and sub-national coverage per mass drug administration reported by Ministries of Health. DHS included maternally-reported deworming status within the past 6 months for each child surveyed. We estimated differences in sub-national deworming coverage using WHO and DHS data, and performed sensitivity analyses.
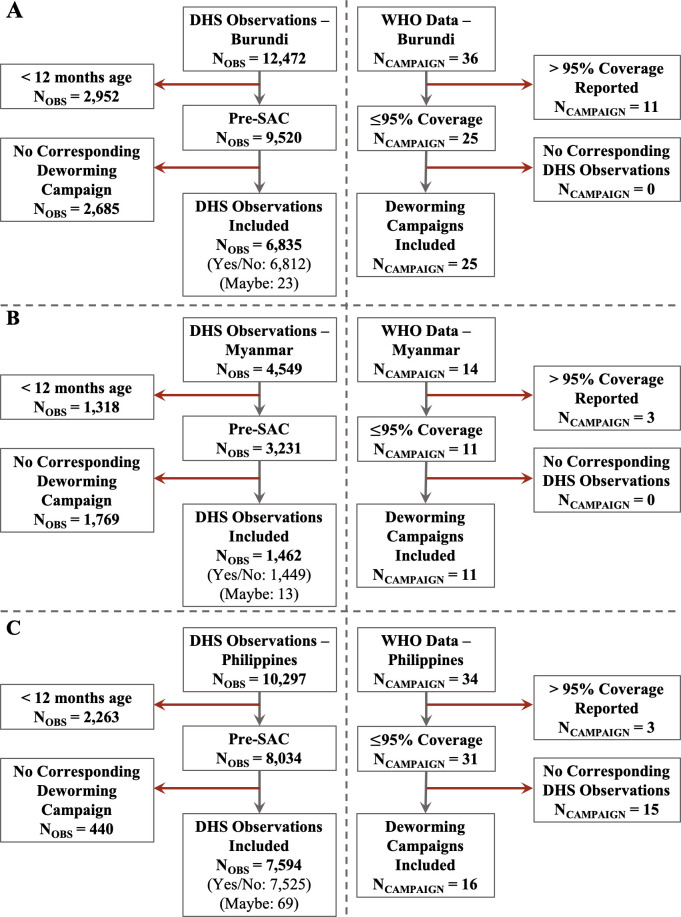
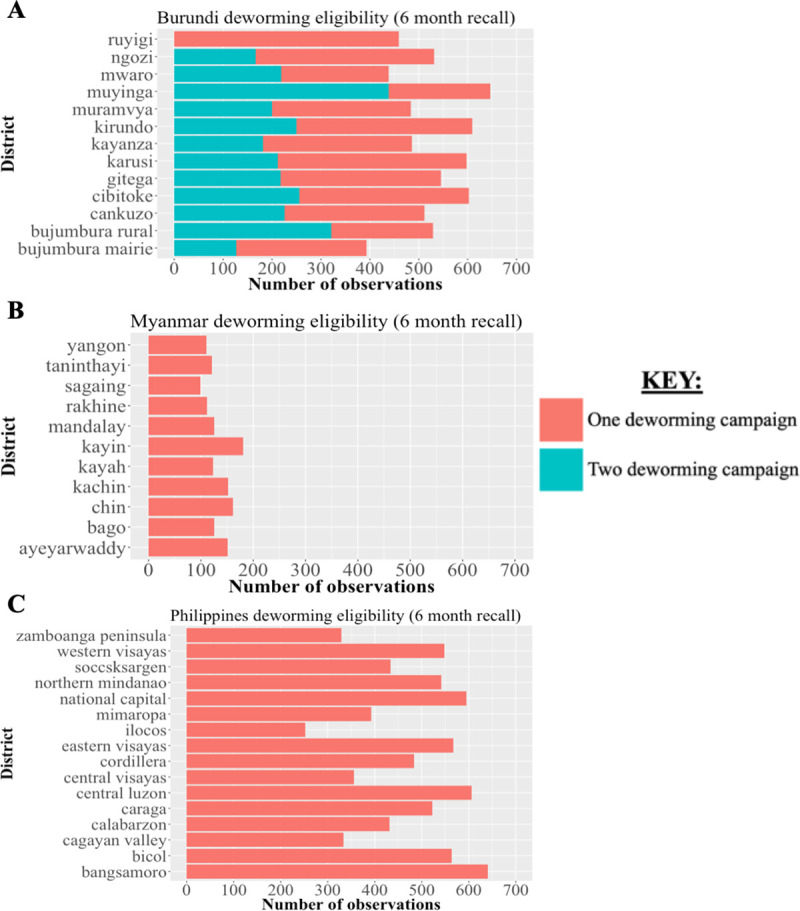
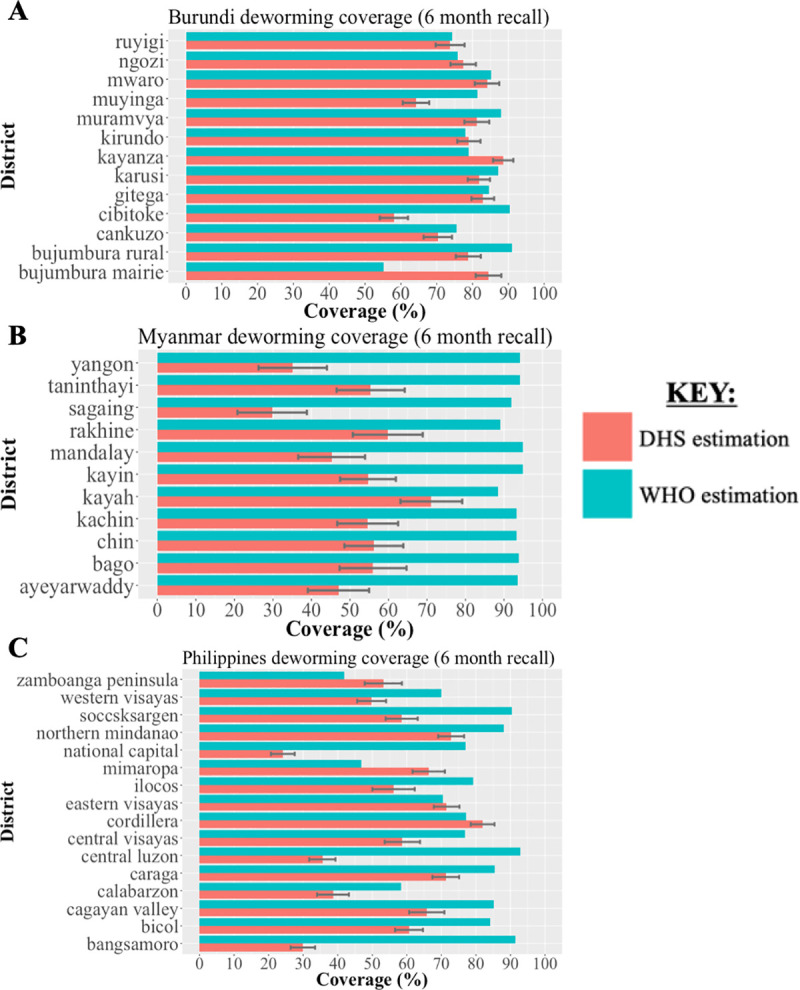
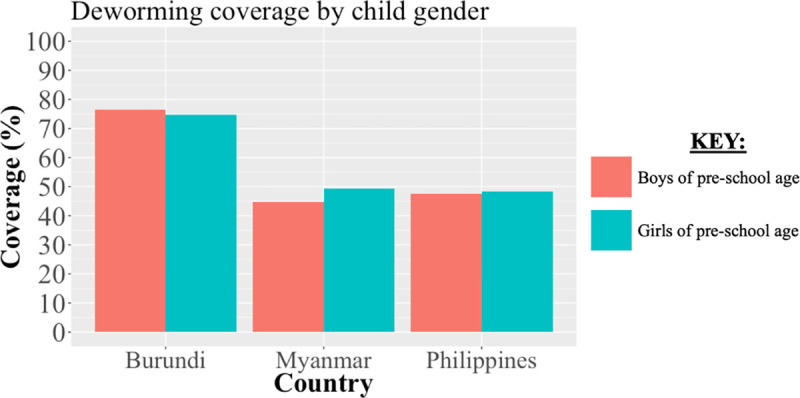
Principal findings: We compared data on pre-school aged children from 13 of 18 districts in Burundi (N = 6,835 in DHS), 11 of 15 districts in Myanmar (N = 1,462 in DHS) and 16 of 17 districts in the Philippines (N = 7,594 in DHS) following data exclusion. The national deworming coverages estimated by DHS in Burundi, Myanmar, and the Philippines were 75.5% (95% CI: 73.7%-77.7%), 47.0% (95% CI: 42.7%-51.3%), and 48.0% (95% CI: 46.0%-50.0%), respectively. The national deworming coverages reported by WHO in Burundi, Myanmar, and the Philippines were 80.1%, 93.6% and 75.7%, respectively. The mean absolute differences in district-level coverage reported to WHO and estimated by DHS in Burundi, Myanmar, and the Philippines were 9.5%, 41.5%, and 24.6%, respectively. Across countries, coverage reported to WHO was frequently higher than DHS estimates (32 of 40 districts). National deworming coverage from DHS estimates were similar by gender within countries.
Conclusions and significance: Agreement of deworming coverage reported to WHO and estimated by DHS data was heterogeneous across countries, varying from broadly compatible in Burundi to largely discrepant in Myanmar. DHS data could complement deworming data reported to WHO to improve data monitoring practices and serve as an independent sub-national source of coverage data.
Conflict of interest statement
NCL, RG, and DGA report funding from the World Health Organization. AM, AM, and PM are employed by the World Health Organization.
Figures
Similar articles
-
Provision of deworming intervention to pregnant women by antenatal services in countries endemic for soil-transmitted helminthiasis.PLoS Negl Trop Dis. 2019 May 13;13(5):e0007406. doi: 10.1371/journal.pntd.0007406. eCollection 2019 May. PLoS Negl Trop Dis. 2019. PMID: 31083673 Free PMC article.
-
Spatiotemporal distribution and population at risk of soil-transmitted helminth infections following an eight-year school-based deworming programme in Burundi, 2007-2014.Parasit Vectors. 2017 Nov 23;10(1):583. doi: 10.1186/s13071-017-2505-x. Parasit Vectors. 2017. PMID: 29169386 Free PMC article.
-
State of deworming coverage and equity in low-income and middle-income countries using household health surveys: a spatiotemporal cross-sectional study.Lancet Glob Health. 2019 Nov;7(11):e1511-e1520. doi: 10.1016/S2214-109X(19)30413-9. Epub 2019 Sep 23. Lancet Glob Health. 2019. PMID: 31558383 Free PMC article.
-
Public health deworming programmes for soil-transmitted helminths in children living in endemic areas.Cochrane Database Syst Rev. 2019 Sep 11;9(9):CD000371. doi: 10.1002/14651858.CD000371.pub7. Cochrane Database Syst Rev. 2019. PMID: 31508807 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
Cited by
-
Disability in childhood and the equity of health services: a cross-sectional comparison of mass drug administration strategies for soil-transmitted helminths in southern Malawi.BMJ Open. 2024 Sep 5;14(9):e083321. doi: 10.1136/bmjopen-2023-083321. BMJ Open. 2024. PMID: 39242171 Free PMC article.
-
Deworming Coverage and its Predictors among Ethiopian Children Aged 24 to 59 Months: Further Analysis of EDHS 2016 Data Set.Glob Pediatr Health. 2021 Jun 11;8:2333794X211022908. doi: 10.1177/2333794X211022908. eCollection 2021. Glob Pediatr Health. 2021. PMID: 34179300 Free PMC article.
-
Review of the neglected tropical diseases programme implementation during 2012-2019 in the WHO-Eastern Mediterranean Region.PLoS Negl Trop Dis. 2022 Sep 29;16(9):e0010665. doi: 10.1371/journal.pntd.0010665. eCollection 2022 Sep. PLoS Negl Trop Dis. 2022. PMID: 36173943 Free PMC article. Review.
-
Overestimation of school-based deworming coverage resulting from school-based reporting.PLoS Negl Trop Dis. 2023 Apr 10;17(4):e0010401. doi: 10.1371/journal.pntd.0010401. eCollection 2023 Apr. PLoS Negl Trop Dis. 2023. PMID: 37036890 Free PMC article.
-
Individual and community level predictors of utilization of deworming medications among pregnant women in Ethiopia: A multilevel analysis.PLoS Negl Trop Dis. 2022 Sep 15;16(9):e0010731. doi: 10.1371/journal.pntd.0010731. eCollection 2022 Sep. PLoS Negl Trop Dis. 2022. PMID: 36107833 Free PMC article.
References
-
- World Health Organization. Accelerating work to overcome the global impact of neglected tropical diseases–A roadmap for implementation [Internet]. World Health Organization; 2012. Available from: https://www.who.int/neglected_diseases/NTD_RoadMap_2012_Fullversion.pdf
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
