

How accurate is the diagnosis of rheumatic fever in Egypt? Data from the national rheumatic heart disease prevention and control program (2006-2018)
- PMID: 32804953
- PMCID: PMC7451991
- DOI: 10.1371/journal.pntd.0008558
How accurate is the diagnosis of rheumatic fever in Egypt? Data from the national rheumatic heart disease prevention and control program (2006-2018)
Abstract
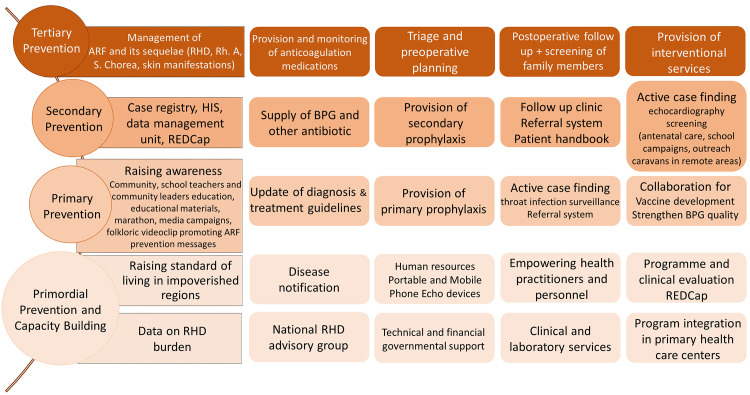
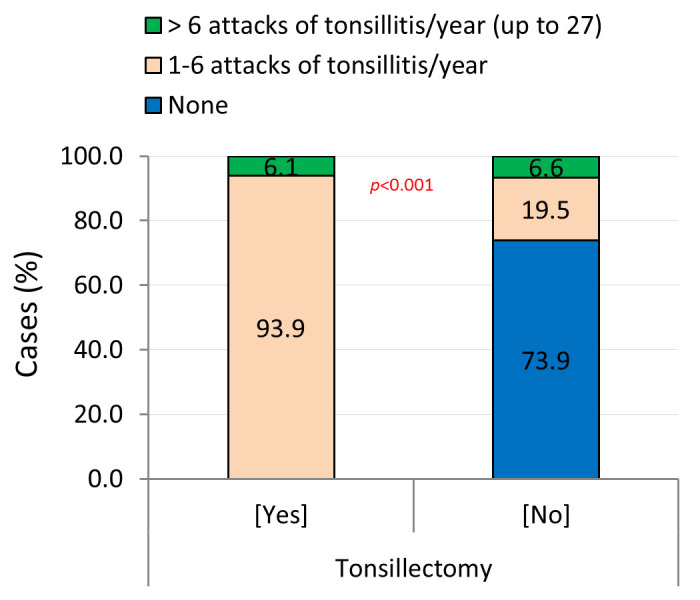
Rheumatic heart disease (RHD) as a chronic sequela of repeated episodes of acute rheumatic fever (ARF), remains a cause of cardiac morbidity in Egypt although it is given full attention through a national RHD prevention and control program. The present report reviews our experience with subjects presenting with ARF or its sequelae in a single RHD centre and describes the disease pattern over the last decade. A cross-sectional study was conducted in El-Mahalla RHD centre between 2006 and 2018. A total of 17014 individual were enrolled and evaluated. Diagnosis ARF was based on the 2015 revised Jones criteria and RHD was ruled in by echocardiography. The majority of the screened subjects were female (63.2%), in the age group 5-15 years (64.6%), rural residents (61.2%), had primary education (43.0%), and of low socioeconomic standard (50.2%). The total percentage of cases presenting with ARF sequelae was 29.3% [carditis/RHD (10.8%), rheumatic arthritis (Rh.A) (14.9%), and Sydenham's chorea (0.05%)]. Noticeably, 72% were free of any cardiac insult, of which 37.7% were victims of misdiagnoses made elsewhere by untrained practitioners who prescribed for them long term injectable long-acting penicillin [Benzathine Penicillin G (BPG)] without need. About 54% of the study cohort reported the occurrence of recurrent attacks of tonsillitis of which 65.2% underwent tonsillectomy. Among those who experienced tonsillectomy and/or received BPG in the past, 14.5% and 22.3% respectively had eventually developed RHD. Screening of family members of some RHD cases who needed cardiac surgery revealed 20.7% with undiagnosed ARF sequalae [RHD (56.0%) and Rh.A (52.2%)]. Upon the follow-up of RHD cases, 1.2% had improved, 98.4% were stable and 0.4% had their heart condition deteriorated. Misdiagnosis of ARF or its sequelae and poor compliance with BPG use may affect efforts being exerted to curtail the disease. Updating national guidelines, capacity building, and reliance on appropriate investigations should be emphasized. Since the genetic basis of RHD is literally confirmed, a family history of RHD warrants screening of all family members for early detection of the disease.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Cunningham MW (2016) Post-streptococcal autoimmune sequelae: Rheumatic fever and beyond. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
