

Effects of Dietary Glycemic Index and Glycemic Load on Cardiometabolic and Reproductive Profiles in Women with Polycystic Ovary Syndrome: A Systematic Review and Meta-analysis of Randomized Controlled Trials
- PMID: 32805007
- PMCID: PMC7850057
- DOI: 10.1093/advances/nmaa092
Effects of Dietary Glycemic Index and Glycemic Load on Cardiometabolic and Reproductive Profiles in Women with Polycystic Ovary Syndrome: A Systematic Review and Meta-analysis of Randomized Controlled Trials
Abstract
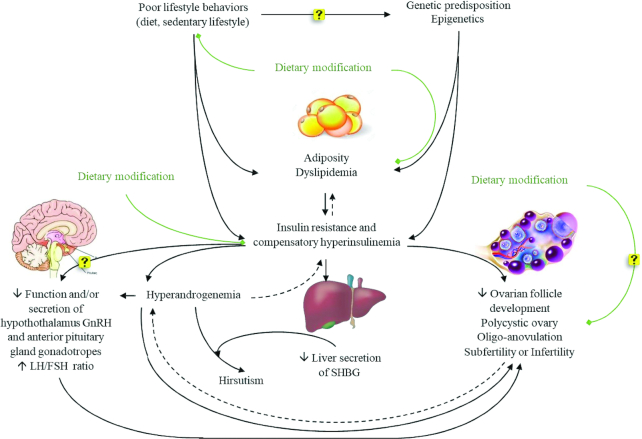
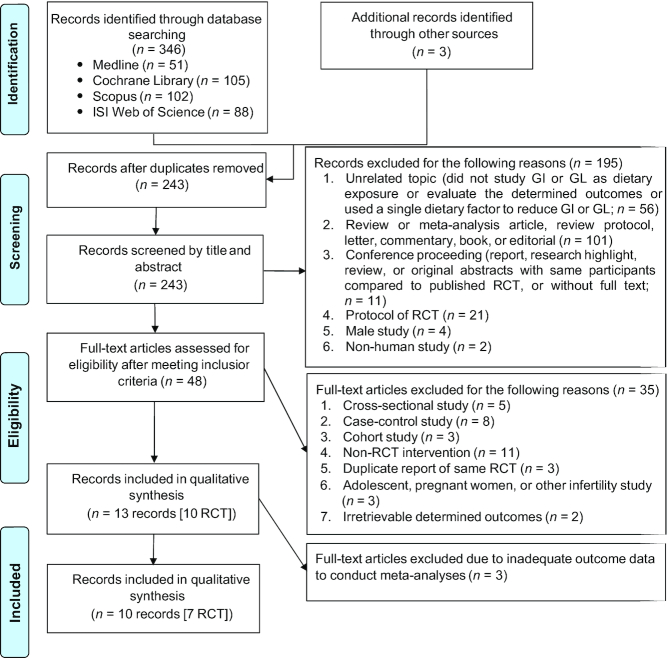
Women with polycystic ovary syndrome (PCOS) exhibit cardiometabolic (e.g., insulin resistance) and associated reproductive disruptions. Lifestyle modification (e.g., diet) is recommended as the first-line therapy to manage PCOS; however, a favorable dietary regimen remains unclear beyond energy restriction. We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) to summarize evidence on impacts of dietary glycemic index (GI) or glycemic load (GL) on cardiometabolic and reproductive profiles to update the International Evidence-based Guideline for the Assessment and Management of PCOS. Databases of MEDLINE, Cochrane, Web of Science, and Scopus were searched through 30 October 2019, and confirmed on 25 March 2020, to identify RCTs (≥8 wk) comparing the effects of diets with lower (LGI/LGL) and higher (HGI/HGL) GI/GL on glucoregulatory outcomes, lipid profile, anthropometrics, and androgen status in PCOS. The primary outcome was HOMA-IR. Data were pooled by random-effects models and expressed as weighted mean differences and 95% CIs. The risk of bias was assessed by the Cochrane tool. Ten RCTs (n = 403) were eligible. Eight evaluated LGI and 2 LGL diets. LGI diets decreased HOMA-IR (-0.78; -1.20, -0.37; I2 = 86.6%), fasting insulin (-2.39; -4.78, 0.00 μIU/mL; I2 = 76.8%), total cholesterol (-11.13; -18.23, -4.04 mg/dL; I2 = 0.0%), LDL cholesterol (-6.27; -12.01, -0.53 mg/dL; I2 = 0.0%), triglycerides (-14.85; -28.75, -0.95 mg/dL; I2 = 31.0%), waist circumference (-2.81; -4.40, -1.23 cm; I2 = 53.9%), and total testosterone (-0.21; -0.32, -0.09 nmol/L; I2 = 8.6%) compared with HGI diets (all: P ≤ 0.05) without affecting fasting glucose, HDL cholesterol, weight, or free androgen index (all: P ≥ 0.07). Some results were contradictory and only described narratively for 2 RCTs that evaluated LGL diets, since inclusion in meta-analyses was not possible. LGI diets improved glucoregulatory outcomes (HOMA-IR, insulin), lipid profiles, abdominal adiposity, and androgen status, conceivably supporting their inclusion for dietary management of PCOS. Further RCTs should confirm these observations and address whether LGI diets improve more patient-pressing complications, including ovulatory cyclicity, infertility, and cardiovascular disease risk in this high-risk population. This review was registered at www.crd.york.ac.uk/PROSPERO as CRD42020175300.
Keywords: cardiovascular diseases; diet; dyslipidemias; glucose; hyperandrogenism; insulin; metabolic diseases; obesity; polycystic ovary syndrome.
Copyright © The Author(s) on behalf of the American Society for Nutrition 2020.
Figures
Similar articles
-
Comparison of dietary and physical activity behaviors in women with and without polycystic ovary syndrome: a systematic review and meta-analysis of 39 471 women.Hum Reprod Update. 2022 Nov 2;28(6):910-955. doi: 10.1093/humupd/dmac023. Hum Reprod Update. 2022. PMID: 35639552 Free PMC article.
-
Effects of nutrition on metabolic and endocrine outcomes in women with polycystic ovary syndrome: an umbrella review of meta-analyses of randomized controlled trials.Nutr Rev. 2023 Apr 11;81(5):555-577. doi: 10.1093/nutrit/nuac075. Nutr Rev. 2023. PMID: 36099162
-
Dietary glycemic index is associated with less favorable anthropometric and metabolic profiles in polycystic ovary syndrome women with different phenotypes.Fertil Steril. 2013 Oct;100(4):1081-8. doi: 10.1016/j.fertnstert.2013.06.005. Epub 2013 Jul 2. Fertil Steril. 2013. PMID: 23830153
-
Efficacy of omega-3 fatty acid supplementation on cardiovascular risk factors in patients with polycystic ovary syndrome: a systematic review and meta-analysis.Ann Palliat Med. 2021 Jun;10(6):6425-6437. doi: 10.21037/apm-21-1050. Ann Palliat Med. 2021. PMID: 34237964
-
Effects of Curcumin on Glycemic Control and Lipid Profile in Polycystic Ovary Syndrome: Systematic Review with Meta-Analysis and Trial Sequential Analysis.Nutrients. 2021 Feb 21;13(2):684. doi: 10.3390/nu13020684. Nutrients. 2021. PMID: 33669954 Free PMC article.
Cited by
-
The Role of the Mediterranean Diet in Assisted Reproduction: A Literature Review.Nutrients. 2024 Aug 22;16(16):2807. doi: 10.3390/nu16162807. Nutrients. 2024. PMID: 39203942 Free PMC article. Review.
-
An update of polycystic ovary syndrome: causes and therapeutics options.Heliyon. 2022 Oct 10;8(10):e11010. doi: 10.1016/j.heliyon.2022.e11010. eCollection 2022 Oct. Heliyon. 2022. PMID: 36267367 Free PMC article.
-
Food insecurity is associated with the sleep quality and quantity in adults: a systematic review and meta-analysis.Public Health Nutr. 2023 Apr;26(4):792-802. doi: 10.1017/S1368980022002488. Epub 2022 Nov 23. Public Health Nutr. 2023. PMID: 36416108 Free PMC article. Review.
-
The Influence of Metabolic Factors and Diet on Fertility.Nutrients. 2023 Feb 27;15(5):1180. doi: 10.3390/nu15051180. Nutrients. 2023. PMID: 36904180 Free PMC article. Review.
-
Role of Omega-3 Fatty Acids in Improving Metabolic Dysfunctions in Polycystic Ovary Syndrome.Nutrients. 2024 Sep 3;16(17):2961. doi: 10.3390/nu16172961. Nutrients. 2024. PMID: 39275277 Free PMC article. Review.
References
-
- March WA, Moore VM, Willson KJ, Phillips DIW, Norman RJ, Davies MJ. The prevalence of polycystic ovary syndrome in a community sample assessed under contrasting diagnostic criteria. Hum Reprod. 2010;25:544–51. - PubMed
-
- Carmina E, Lobo RA. Polycystic ovary syndrome (PCOS): arguably the most common endocrinopathy is associated with significant morbidity in women. J Clin Endocrinol Metab. 1999;84:1897–9. - PubMed
-
- Wild RA, Carmina E, Diamanti-Kandarakis E, Dokras A, Escobar-Morreale HF, Futterweit W, Lobo R, Norman RJ, Talbott E, Dumesic DA. Assessment of cardiovascular risk and prevention of cardiovascular disease in women with the polycystic ovary syndrome: a consensus statement by the Androgen Excess and Polycystic Ovary Syndrome (AE-PCOS) Society. J Clin Endocrinol Metab. 2010;95:2038–49. - PubMed
-
- Kazemi M, Pierson RA, Lujan ME, Chilibeck PD, McBreairty LE, Gordon JJ, Serrao SB, Zello GA, Chizen DR. Comprehensive evaluation of type 2 diabetes and cardiovascular disease risk profiles in reproductive-age women with polycystic ovary syndrome: a large Canadian cohort. J Obstet Gynaecol Can. 2019;41:1453–60. - PubMed
-
- Kazemi M, Jarrett BY, Parry SA, Thalacker-Mercer A, Hoeger KM, Spandorfer SD, Lujan ME. Osteosarcopenia in reproductive-aged women with polycystic ovary syndrome: a multicenter case-control study. J Clin Endocrinol Metab. 2020. [Cited July 3, 2020]. Available from: 10.1210/clinem/dgaa426. - DOI - PMC - PubMed
