

The National COVID Cohort Collaborative (N3C): Rationale, design, infrastructure, and deployment
- PMID: 32805036
- PMCID: PMC7454687
- DOI: 10.1093/jamia/ocaa196
The National COVID Cohort Collaborative (N3C): Rationale, design, infrastructure, and deployment
Abstract
Objective: Coronavirus disease 2019 (COVID-19) poses societal challenges that require expeditious data and knowledge sharing. Though organizational clinical data are abundant, these are largely inaccessible to outside researchers. Statistical, machine learning, and causal analyses are most successful with large-scale data beyond what is available in any given organization. Here, we introduce the National COVID Cohort Collaborative (N3C), an open science community focused on analyzing patient-level data from many centers.
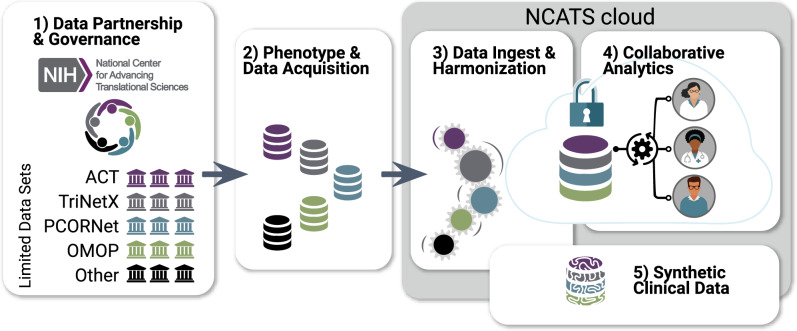
Materials and methods: The Clinical and Translational Science Award Program and scientific community created N3C to overcome technical, regulatory, policy, and governance barriers to sharing and harmonizing individual-level clinical data. We developed solutions to extract, aggregate, and harmonize data across organizations and data models, and created a secure data enclave to enable efficient, transparent, and reproducible collaborative analytics.
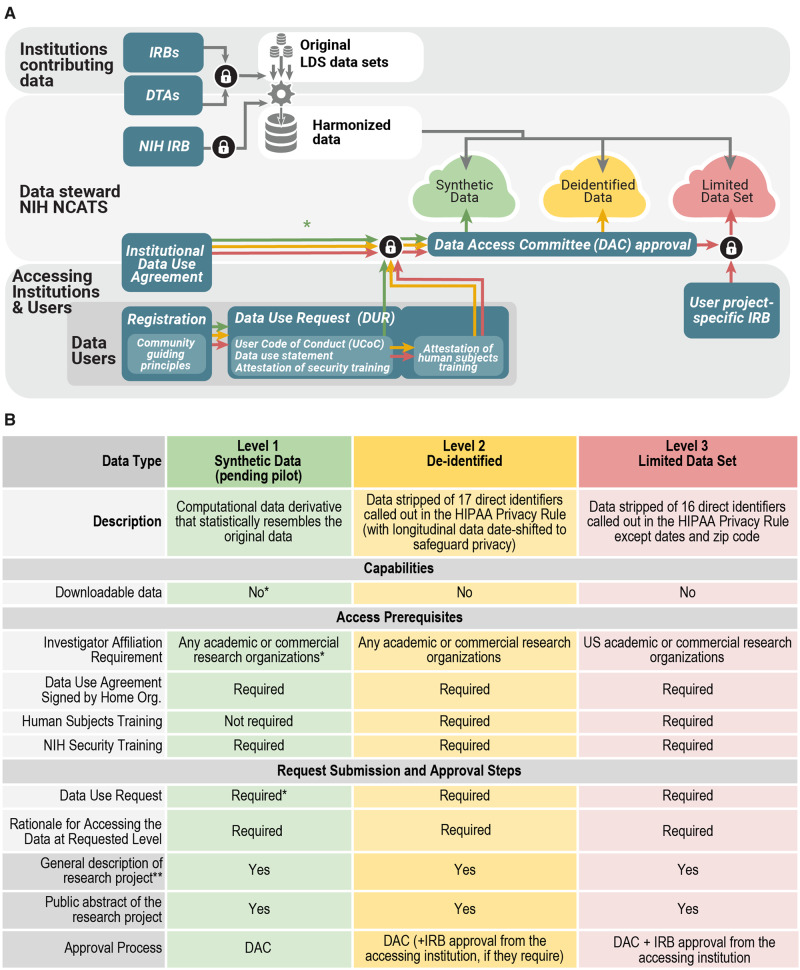
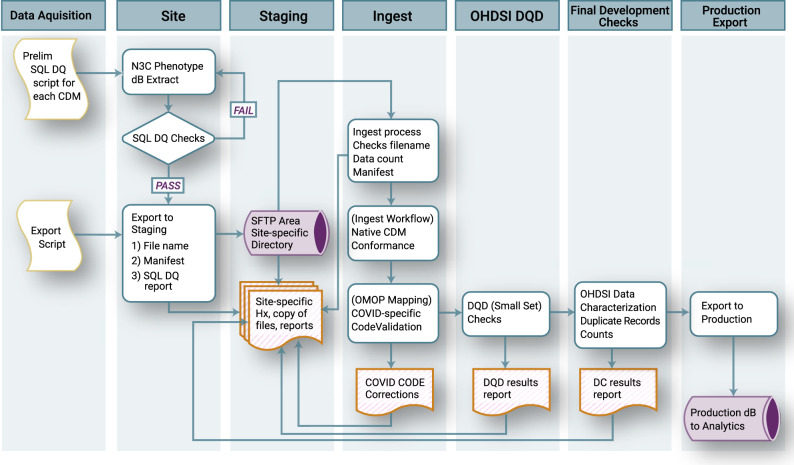
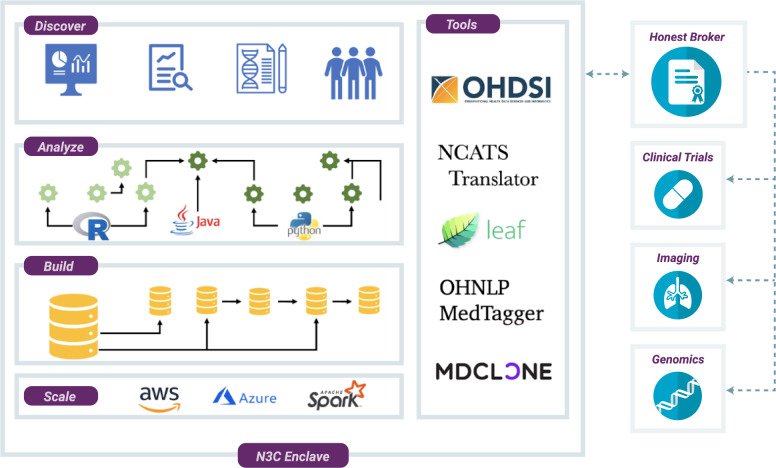
Results: Organized in inclusive workstreams, we created legal agreements and governance for organizations and researchers; data extraction scripts to identify and ingest positive, negative, and possible COVID-19 cases; a data quality assurance and harmonization pipeline to create a single harmonized dataset; population of the secure data enclave with data, machine learning, and statistical analytics tools; dissemination mechanisms; and a synthetic data pilot to democratize data access.
Conclusions: The N3C has demonstrated that a multisite collaborative learning health network can overcome barriers to rapidly build a scalable infrastructure incorporating multiorganizational clinical data for COVID-19 analytics. We expect this effort to save lives by enabling rapid collaboration among clinicians, researchers, and data scientists to identify treatments and specialized care and thereby reduce the immediate and long-term impacts of COVID-19.
Keywords: COVID-19; EHR data; SARS-CoV-2; clinical data model harmonization; collaborative analytics; open science.
© The Author(s) 2020. Published by Oxford University Press on behalf of the American Medical Informatics Association.
Figures
References
-
- Johns Hopkins Coronavirus Resource Center. COVID-19 Map. https://coronavirus.jhu.edu/map.html Accessed July 12, 2020.
