

Compliance Phenotypes in Early Acute Respiratory Distress Syndrome before the COVID-19 Pandemic
- PMID: 32805143
- PMCID: PMC7605177
- DOI: 10.1164/rccm.202005-2046OC
Compliance Phenotypes in Early Acute Respiratory Distress Syndrome before the COVID-19 Pandemic
Abstract
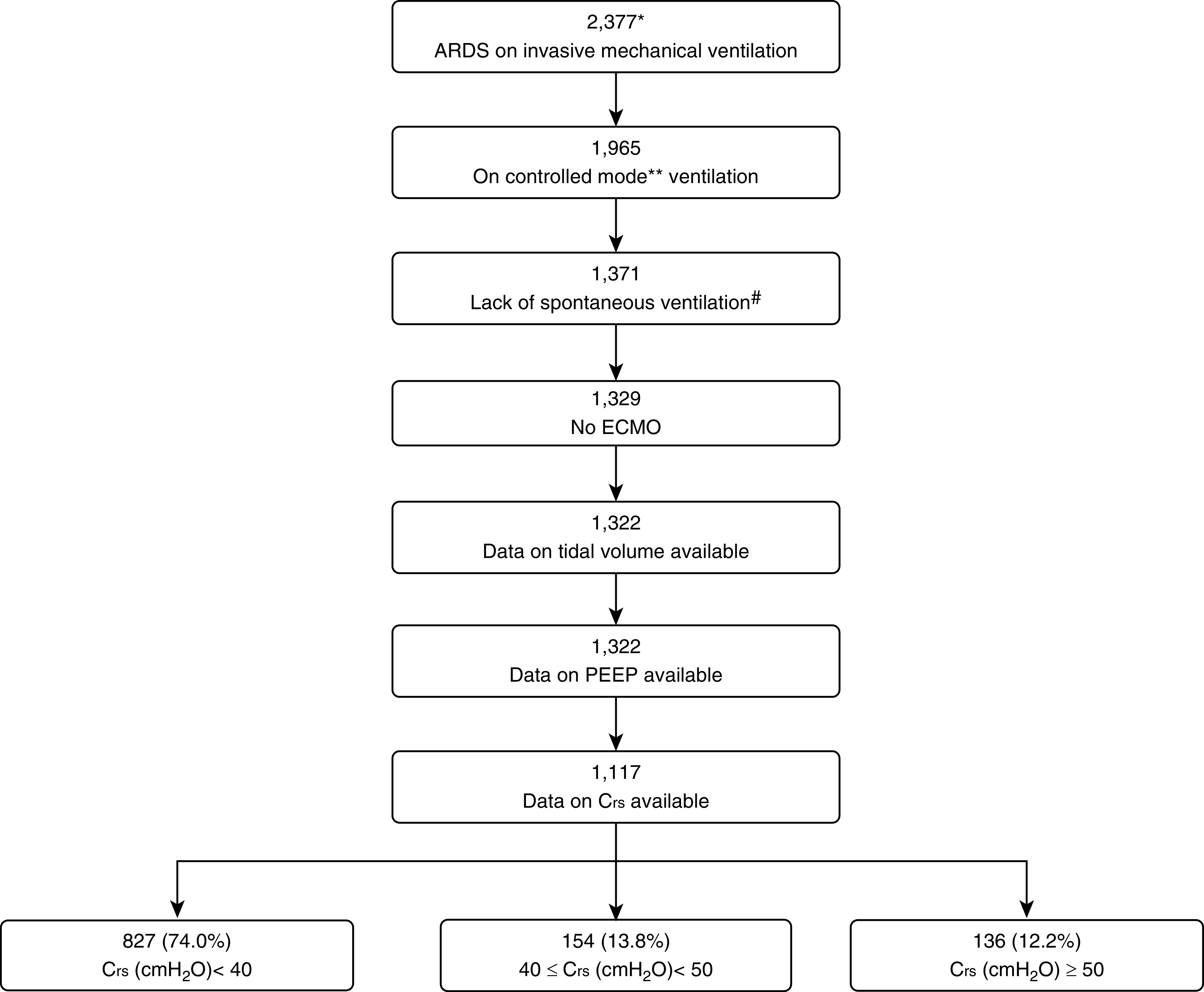
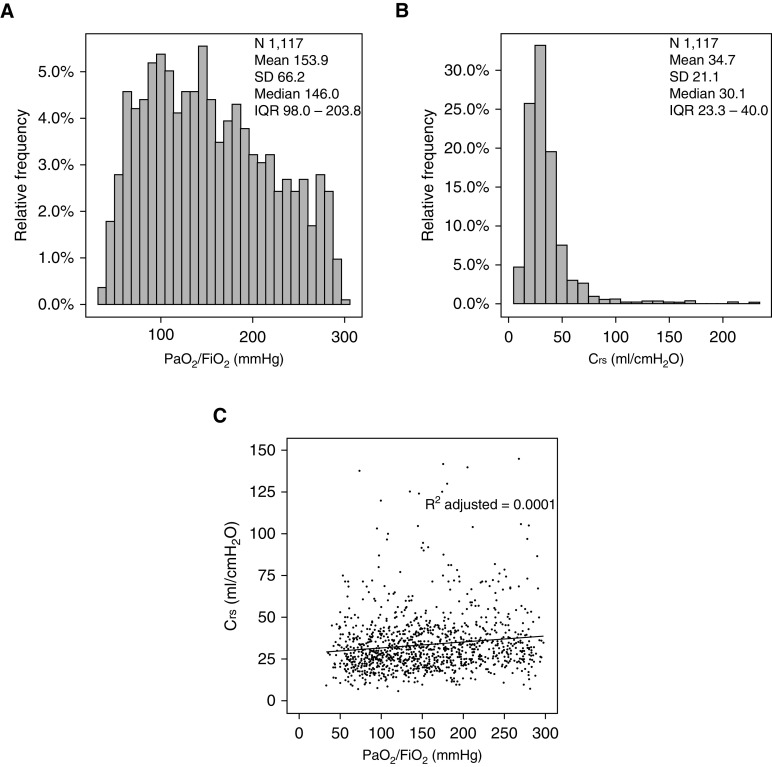
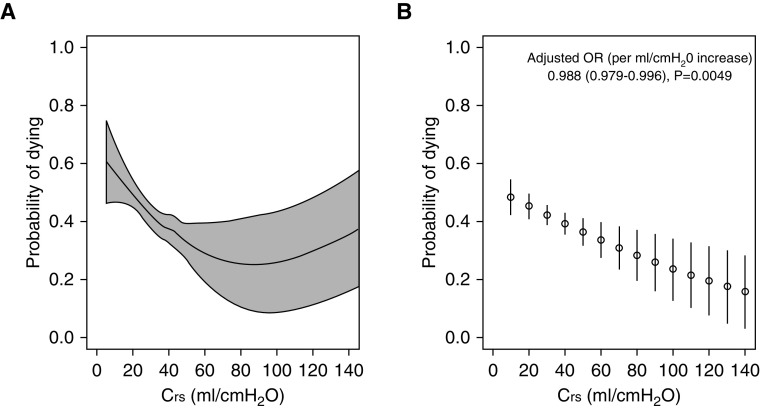
Rationale: A novel model of phenotypes based on set thresholds of respiratory system compliance (Crs) was recently postulated in context of coronavirus disease (COVID-19) acute respiratory distress syndrome (ARDS). In particular, the dissociation between the degree of hypoxemia and Crs was characterized as a distinct ARDS phenotype.Objectives: To determine whether such Crs-based phenotypes existed among patients with ARDS before the COVID-19 pandemic and to closely examine the Crs-mortality relationship.Methods: We undertook a secondary analysis of patients with ARDS, who were invasively ventilated on controlled modes and enrolled in a large, multinational, epidemiological study. We assessed Crs, degree of hypoxemia, and associated Crs-based phenotypic patterns with their characteristics and outcomes.Measurements and Main Results: Among 1,117 patients with ARDS who met inclusion criteria, the median Crs was 30 (interquartile range, 23-40) ml/cm H2O. One hundred thirty-six (12%) patients had preserved Crs (≥50 ml/cm H2O; phenotype with low elastance ["phenotype L"]), and 827 (74%) patients had poor Crs (<40 ml/cm H2O; phenotype with high elastance ["phenotype H"]). Compared with those with phenotype L, patients with phenotype H were sicker and had more comorbidities and higher hospital mortality (32% vs. 45%; P < 0.05). A near complete dissociation between PaO2/FiO2 and Crs was observed. Of 136 patients with phenotype L, 58 (43%) had a PaO2/FiO2 < 150. In a multivariable-adjusted analysis, the Crs was independently associated with hospital mortality (adjusted odds ratio per ml/cm H2O increase, 0.988; 95% confidence interval, 0.979-0.996; P = 0.005).Conclusions: A wide range of Crs was observed in non-COVID-19 ARDS. Approximately one in eight patients had preserved Crs. PaO2/FiO2 and Crs were dissociated. Lower Crs was independently associated with higher mortality. The Crs-mortality relationship lacked a clear transition threshold.
Keywords: acute respiratory distress syndrome; intensive care; mechanical ventilation; phenotype; respiratory system compliance.
Figures
Comment in
-
Novel Phenotypes in Respiratory Failure: Same As It Ever Was.Am J Respir Crit Care Med. 2020 Nov 1;202(9):1207-1209. doi: 10.1164/rccm.202008-3322ED. Am J Respir Crit Care Med. 2020. PMID: 32926789 Free PMC article. No abstract available.
References
-
- Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, et al. ARDS Definition Task Force. Acute respiratory distress syndrome: the Berlin definition. JAMA. 2012;307:2526–2533. - PubMed
-
- Henderson WR, Chen L, Amato MBP, Brochard LJ. Fifty years of research in ARDS: respiratory mechanics in acute respiratory distress syndrome. Am J Respir Crit Care Med. 2017;196:822–833. - PubMed
-
- Gattinoni L, Pesenti A, Avalli L, Rossi F, Bombino M. Pressure-volume curve of total respiratory system in acute respiratory failure: computed tomographic scan study. Am Rev Respir Dis. 1987;136:730–736. - PubMed
-
- Amato MB, Meade MO, Slutsky AS, Brochard L, Costa EL, Schoenfeld DA, et al. Driving pressure and survival in the acute respiratory distress syndrome. N Engl J Med. 2015;372:747–755. - PubMed
-
- Nuckton TJ, Alonso JA, Kallet RH, Daniel BM, Pittet JF, Eisner MD, et al. Pulmonary dead-space fraction as a risk factor for death in the acute respiratory distress syndrome. N Engl J Med. 2002;346:1281–1286. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
