

Differential diagnosis of orthostatic hypotension
- PMID: 32805514
- PMCID: PMC7502506
- DOI: 10.1016/j.autneu.2020.102713
Differential diagnosis of orthostatic hypotension
Abstract
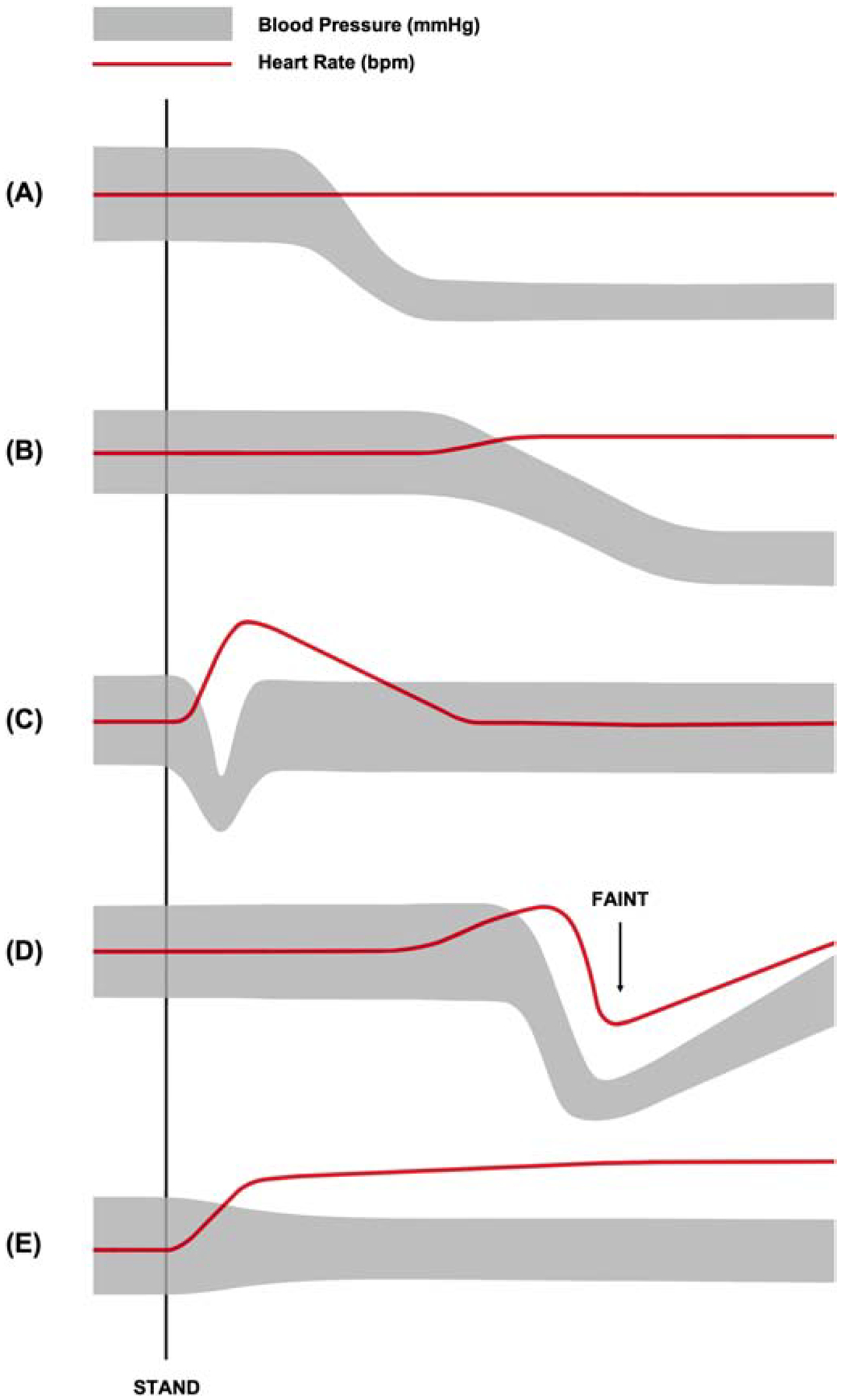
Orthostatic hypotension (OH) is a common clinical manifestation characterized by a significant fall in blood pressure with postural change and is frequently accompanied by debilitating symptoms of orthostatic intolerance. The reported prevalence of OH ranges between 5 and 10% in middle-aged adults with a burden that increases concomitantly with age; in those over 60 years of age, the prevalence is estimated to be over 20%. Unfortunately, the clinical course of OH is not necessarily benign. OH patients are at an increased risk of adverse clinical outcomes including death, falls, cardiovascular and cerebrovascular events, syncope, and impaired quality of life. The differential diagnosis of OH is broad and includes acute precipitants as well as chronic underlying medical conditions, especially of neurological origin. Appropriate diagnosis relies on a systematic history and physical examination with particular attention to orthostatic vital signs, keeping in mind that ambient conditions during diagnostic testing may affect OH detection due to factors such as diurnal variation.
Keywords: Delayed orthostatic hypotension; Initial orthostatic hypotension; Neurogenic orthostatic hypotension; Orthostatic hypotension; Postural orthostatic tachycardia syndrome; Vasovagal syncope.
Copyright © 2020 Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of competing interest SRR is a consultant to Lundbeck LLC and Theravance Biopharma related to neurogenic orthostatic hypotension, and has received honoraria from the Academy for Continued Healthcare Learning and Medscape for developing continuing medical educational materials about neurogenic orthostatic hypotension. He also serves as DMSB Chair for a Phase 2 study of an irritable bowel syndrome medication for Arena Pharmaceuticals with compensation. SRR is currently the President of the American Autonomic Society without financial compensation.
Figures
Similar articles
-
[Syndromes of autonomic insufficiency associated with orthostatic intolerance: classification, diagnostic and therapeutic approach].Z Kardiol. 1999 Aug;88(8):541-9. doi: 10.1007/s003920050323. Z Kardiol. 1999. PMID: 10506389 Review. German.
-
Tilt Test: A Review.J Clin Neurophysiol. 2021 Jul 1;38(4):279-286. doi: 10.1097/WNP.0000000000000625. J Clin Neurophysiol. 2021. PMID: 34009851 Review.
-
Dysautonomia: A Forgotten Condition - Part 1.Arq Bras Cardiol. 2021 Apr;116(4):814-835. doi: 10.36660/abc.20200420. Arq Bras Cardiol. 2021. PMID: 33886735 Free PMC article. English, Portuguese.
-
Pathophysiology, diagnosis, and treatment of orthostatic hypotension and vasovagal syncope.Cardiol Rev. 2008 Jan-Feb;16(1):4-20. doi: 10.1097/CRD.0b013e31815c8032. Cardiol Rev. 2008. PMID: 18091397 Review.
-
Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome.Auton Neurosci. 2011 Apr 26;161(1-2):46-8. doi: 10.1016/j.autneu.2011.02.004. Epub 2011 Mar 9. Auton Neurosci. 2011. PMID: 21393070 No abstract available.
References
-
- Freeman R, Wieling W, Axelrod FB, Benditt DG, Benarroch E, Biaggioni I, et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Clin Auton Res. 2011;21(2):69–72. - PubMed
-
- Ricci F, De Caterina R, Fedorowski A. Orthostatic hypotension: Epidemiology, prognosis, and treatment. J Am Coll Cardiol. 2015;66(7):848–60. - PubMed
-
- Freeman R, Abuzinadah AR, Gibbons C, Jones P, Miglis MG, Sinn DI. Orthostatic Hypotension. J Am Coll Cardiol. 2018;72(11):1294–309. - PubMed
-
- Adalbert R, Coleman MP. Review: Axon pathology in age-related neurodegenerative disorders. Neuropathol Appl Neurobiol. 2013;39(2):90–108. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
