

Neurological outcome after extracorporeal cardiopulmonary resuscitation for in-hospital cardiac arrest: a systematic review and meta-analysis
- PMID: 32807207
- PMCID: PMC7430015
- DOI: 10.1186/s13054-020-03201-0
Neurological outcome after extracorporeal cardiopulmonary resuscitation for in-hospital cardiac arrest: a systematic review and meta-analysis
Abstract
Background: In-hospital cardiac arrest (IHCA) is a major adverse event with a high mortality rate if not treated appropriately. Extracorporeal cardiopulmonary resuscitation (ECPR), as adjunct to conventional cardiopulmonary resuscitation (CCPR), is a promising technique for IHCA treatment. Evidence pertaining to neurological outcomes after ECPR is still scarce.
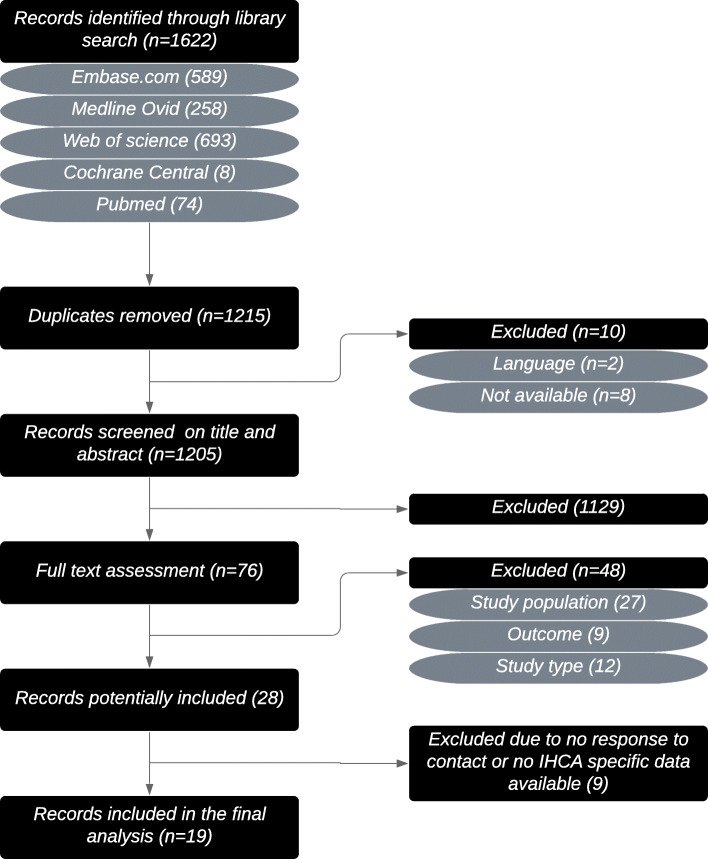
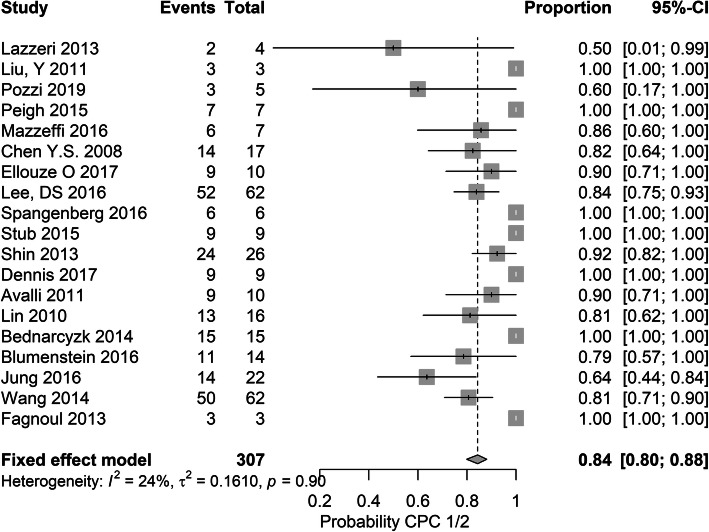
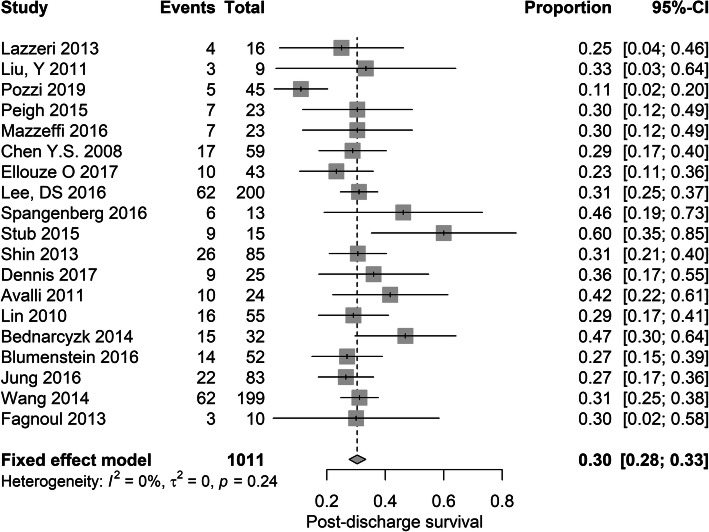
Methods: We performed a comprehensive systematic search of all studies up to December 20, 2019. Our primary outcome was neurological outcome after ECPR at any moment after hospital discharge, defined by the Cerebral Performance Category (CPC) score. A score of 1 or 2 was defined as favourable outcome. Our secondary outcome was post-discharge mortality. A fixed-effects meta-analysis was performed.
Results: Our search yielded 1215 results, of which 19 studies were included in this systematic review. The average survival rate was 30% (95% CI 28-33%, I2 = 0%, p = 0.24). In the surviving patients, the pooled percentage of favourable neurological outcome was 84% (95% CI 80-88%, I2 = 24%, p = 0.90).
Conclusion: ECPR as treatment for in-hospital cardiac arrest is associated with a large proportion of patients with good neurological outcome. The large proportion of favourable outcome could potentially be explained by the selection of patients for treatment using ECPR. Moreover, survival is higher than described in the conventional CPR literature. As indications for ECPR might extend to older or more fragile patient populations in the future, research should focus on increasing survival, while maintaining optimal neurological outcome.
Keywords: Brain injury; CPC; Cerebral performance category; ECPR; In-hospital cardiac arrest; Neurological outcome.
Conflict of interest statement
The authors declare to have no conflict of interest.
Figures
References
-
- Zhu A, Zhang J. Meta-analysis of outcomes of the 2005 and 2010 cardiopulmonary resuscitation guidelines for adults with in-hospital cardiac arrest. Am J Emerg Med. 2016;34:1133–1139. - PubMed
-
- Schluep M, Gravesteijn BY, Stolker RJ, Endeman H, Hoeks SE. One-year survival after in-hospital cardiac arrest: a systematic review and meta-analysis. Resuscitation. 2018;132:90–100. - PubMed
-
- Chen YS, Chao A, Yu HY, Ko WJ, Wu IH, Chen RJC, et al. Analysis and results of prolonged resuscitation in cardiac arrest patients rescued by extracorporeal membrane oxygenation. J Am Coll Cardiol. 2003;41:197–203. - PubMed
-
- ELSO ECPR Supplement to the ELSO General Guidelines Extracorporeal Life Support Organization (ELSO) Guidelines for ECPR Cases. 2013.
-
- Soar J, Nolan JP, Böttiger BW, Perkins GD, Lott C, Carli P, et al. European resuscitation council guidelines for resuscitation 2015. Section 3. Adult advanced life support. Resuscitation. 2015;95:100–147. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
