

Patterns of Cancer Progression of Metastatic Hormone-sensitive Prostate Cancer in the ECOG3805 CHAARTED Trial
- PMID: 32807727
- PMCID: PMC7738423
- DOI: 10.1016/j.euo.2020.07.001
Patterns of Cancer Progression of Metastatic Hormone-sensitive Prostate Cancer in the ECOG3805 CHAARTED Trial
Abstract
Background: ECOG3805 is a randomized trial of testosterone suppression with or without docetaxel for metastatic hormone-sensitive prostate cancer (mHSPC). Deeper prostate-specific antigen (PSA) suppression is prognostic for outcome. However, the concordance of PSA rise and radiographic progression has not been examined previously in mHSPC, whereas this has been reported in metastatic castration-resistant prostate cancer.
Objective: To determine the patterns of progression by PSA and radiographic parameters in patients in ECOG3805.
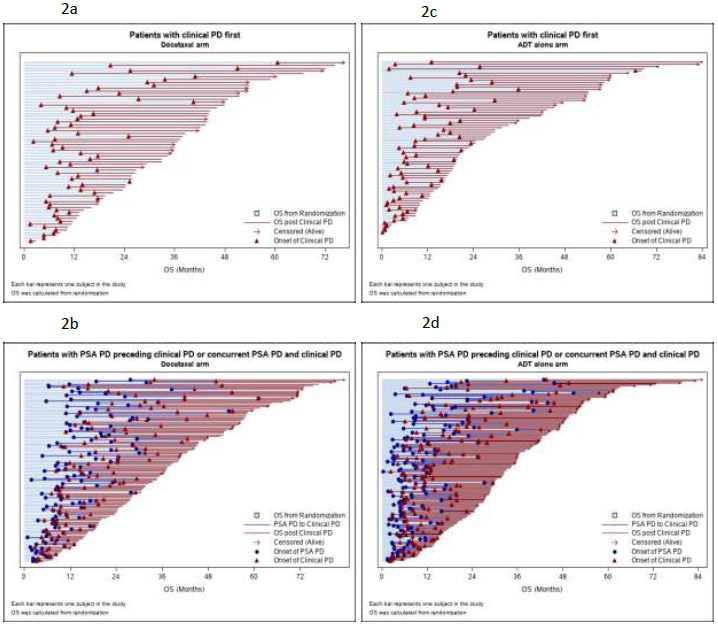
Design, setting, and participants: We conducted a retrospective analysis of all patients in ECOG3805. Patients were classified according to the PSA level at progression (whether PSA level was below 2.0 ng/mL or not) and the type of progression event in the study (either PSA progression as defined by the study with or without clinical progression, or clinical progression alone). Baseline demographics, clinical outcomes, and patterns of progression were compared between the groups.
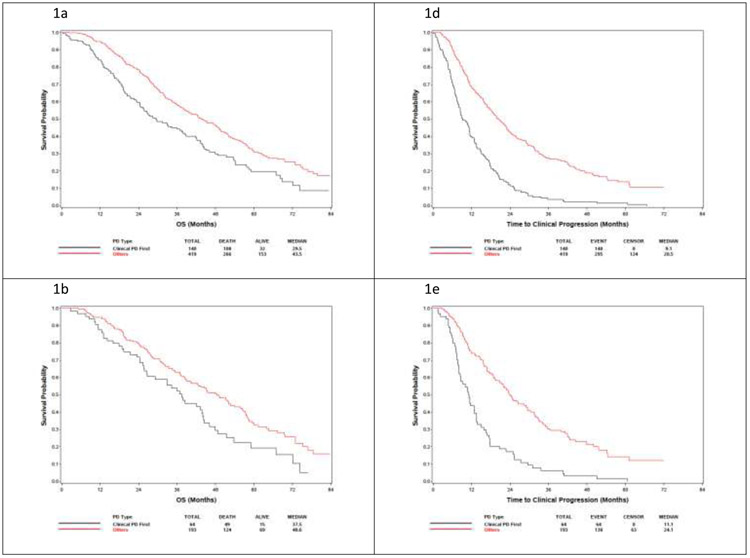
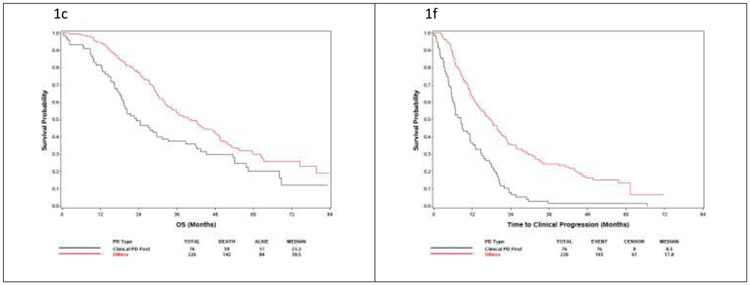
Results and limitations: One in eight patients had clinical progression below a PSA level of 2 ng/mL, and approximately 25% developed clinical progression in the absence of confirmed PSA progression. Overall survival from randomization was shorter in patients with clinical progression without confirmed PSA progression than in patients with PSA progression alone as the first progression. Patient demographics at study entry were not predictive of the pattern of progression. Study limitations include its retrospective and post hoc nature.
Conclusions: Clinical progression prior to PSA rise or at low PSA levels is a relatively frequent phenomenon in mHSPC and is associated with poorer overall survival. Further biological and clinical studies of these patients are warranted.
Patient summary: Reliance on prostate-specific antigen (PSA) alone is an inadequate strategy to monitor patients undergoing treatment for metastatic hormone-sensitive prostate cancer. Prostate cancer can get worse on scans even with low PSA and/or no or small changes in PSA. Imaging should be added to PSA testing to monitor patients with metastatic prostate cancer.
Keywords: Chemotherapy; Clinical trial; Hormone therapy; Prostate cancer; Prostate-specific antigen.
Copyright © 2020 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Opening a Scan of Worms.Eur Urol Oncol. 2020 Dec;3(6):725-727. doi: 10.1016/j.euo.2020.10.009. Epub 2020 Oct 31. Eur Urol Oncol. 2020. PMID: 33139238 No abstract available.
Similar articles
-
Deep and Durable Prostate-specific Antigen Response to Darolutamide with Androgen Deprivation Therapy and Docetaxel, and Association with Clinical Outcomes for Patients with High- or Low-volume Metastatic Hormone-sensitive Prostate Cancer: Analyses of the Randomized Phase 3 ARASENS Study.Eur Urol. 2024 Oct;86(4):329-339. doi: 10.1016/j.eururo.2024.03.036. Epub 2024 Apr 21. Eur Urol. 2024. PMID: 38644146 Clinical Trial.
-
Seven-Month Prostate-Specific Antigen Is Prognostic in Metastatic Hormone-Sensitive Prostate Cancer Treated With Androgen Deprivation With or Without Docetaxel.J Clin Oncol. 2018 Feb 1;36(4):376-382. doi: 10.1200/JCO.2017.75.3921. Epub 2017 Dec 20. J Clin Oncol. 2018. PMID: 29261442 Free PMC article. Clinical Trial.
-
Comparative assessment of docetaxel for safety and efficacy between hormone-sensitive and castration-resistant metastatic prostate cancer.Urol Oncol. 2019 Dec;37(12):999-1005. doi: 10.1016/j.urolonc.2019.07.005. Epub 2019 Jul 31. Urol Oncol. 2019. PMID: 31377168
-
Hormone naïve prostate cancer: predicting and maximizing response intervals.Asian J Androl. 2015 Nov-Dec;17(6):929-35; discussion 933. doi: 10.4103/1008-682X.152821. Asian J Androl. 2015. PMID: 26112479 Free PMC article. Review.
-
Management of Metastatic Hormone-Sensitive Prostate Cancer (mHSPC): an Evolving Treatment Paradigm.Curr Treat Options Oncol. 2019 Jul 9;20(9):69. doi: 10.1007/s11864-019-0668-8. Curr Treat Options Oncol. 2019. PMID: 31286275 Review.
Cited by
-
Feasibility of Monitoring Response to Metastatic Prostate Cancer Treatment with a Methylation-Based Circulating Tumor DNA Approach.Cancers (Basel). 2024 Jan 23;16(3):482. doi: 10.3390/cancers16030482. Cancers (Basel). 2024. PMID: 38339235 Free PMC article.
-
Clinical value of circulating splicing factors in prostate cancer: SRRM1 as a novel predictive biomarker and therapeutic target.Mol Ther Oncol. 2024 Nov 23;32(4):200910. doi: 10.1016/j.omton.2024.200910. eCollection 2024 Dec 19. Mol Ther Oncol. 2024. PMID: 39758250 Free PMC article.
-
Organoids: An Emerging Precision Medicine Model for Prostate Cancer Research.Int J Mol Sci. 2024 Jan 16;25(2):1093. doi: 10.3390/ijms25021093. Int J Mol Sci. 2024. PMID: 38256166 Free PMC article. Review.
-
Circulating Tumor DNA in Prostate Cancer: A Dual Perspective on Early Detection and Advanced Disease Management.Cancers (Basel). 2025 Aug 6;17(15):2589. doi: 10.3390/cancers17152589. Cancers (Basel). 2025. PMID: 40805284 Free PMC article. Review.
-
ΔBSIJ: a quantitative marker for early detection of medication-related osteonecrosis of the jaw in patients with prostate cancer receiving bone-modifying agents.Ann Nucl Med. 2025 Jul 3. doi: 10.1007/s12149-025-02078-9. Online ahead of print. Ann Nucl Med. 2025. PMID: 40608250
References
Publication types
MeSH terms
Substances
Grants and funding
- UG1 CA189829/CA/NCI NIH HHS/United States
- UG1 CA233320/CA/NCI NIH HHS/United States
- U10 CA180795/CA/NCI NIH HHS/United States
- UG1 CA232760/CA/NCI NIH HHS/United States
- UG1 CA233196/CA/NCI NIH HHS/United States
- U10 CA180794/CA/NCI NIH HHS/United States
- U10 CA180888/CA/NCI NIH HHS/United States
- U10 CA180853/CA/NCI NIH HHS/United States
- U10 CA180802/CA/NCI NIH HHS/United States
- UG1 CA233234/CA/NCI NIH HHS/United States
- U10 CA180821/CA/NCI NIH HHS/United States
- U10 CA180801/CA/NCI NIH HHS/United States
- UG1 CA233277/CA/NCI NIH HHS/United States
- U10 CA180790/CA/NCI NIH HHS/United States
- UG1 CA233180/CA/NCI NIH HHS/United States
- U10 CA180820/CA/NCI NIH HHS/United States
- U10 CA180833/CA/NCI NIH HHS/United States
- U10 CA180799/CA/NCI NIH HHS/United States
- U10 CA180867/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
