

Pharmacologic effects of oseltamivir in immunocompromised adult patients as assessed by population PK/PD analysis and drug-disease modelling for dosing regimen optimization
- PMID: 32808306
- PMCID: PMC8246794
- DOI: 10.1111/bcp.14523
Pharmacologic effects of oseltamivir in immunocompromised adult patients as assessed by population PK/PD analysis and drug-disease modelling for dosing regimen optimization
Abstract
Aim: Pharmacologic effects were analysed to determine a dose recommendation for oseltamivir in immunocompromised (IC) adults with influenza.
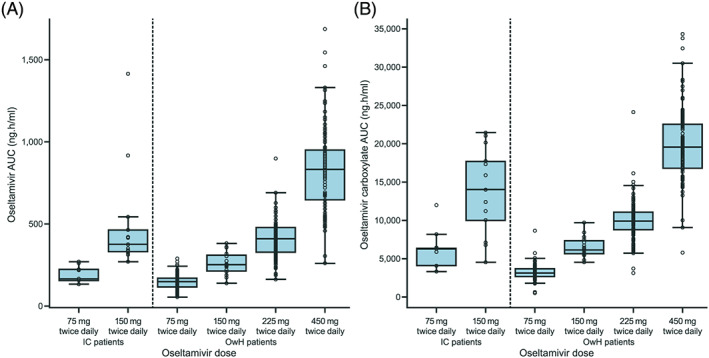
Methods: Quantitative clinical pharmacology methods were applied to data from 160 adult IC patients (aged 18-78 years) from two studies (NV20234, 150 patients; NV25118, 10 patients) who received oseltamivir 75-200 mg twice daily for up to 10 days. An established population-pharmacokinetic (PK) model with additional effects on oseltamivir and oseltamivir carboxylate (OC) clearance described the PK characteristics of oseltamivir in IC patients versus otherwise healthy (OwH) patients from previous clinical trials. Estimated PK parameters were used to evaluate exposure-response relationships for virologic endpoints (time to cessation of viral shedding, viral load measures and treatment-emergent resistance). A drug-disease model characterized the viral kinetics of influenza accounting for the effect of OC on viral production.
Results: Oseltamivir clearance was 32.5% lower (95% confidence interval [CI], 26.1-38.8) and OC clearance was 33.7% lower (95% CI, 23.2-44.1) in IC versus OwH patients. No notable exposure-response relationships were identified for exposures higher than those achieved after conventional dose oseltamivir 75 mg, which appeared to be close to the maximum effect of oseltamivir. Simulations of the drug-disease model predicted that initiating treatment within 48 hours of symptom onset had maximum impact, and a treatment duration of 10 days was favourable over 3-5 days to limit viral rebound.
Conclusions: Our findings support the use of conventional-dose oseltamivir 75 mg twice daily for 10 days in the treatment of IC adult patients with influenza.
Keywords: clinical trials; immunosuppression; modelling and simulation; pharmacokinetic-pharmacodynamic; population analysis.
© 2020 The Authors. British Journal of Clinical Pharmacology published by John Wiley & Sons Ltd on behalf of British Pharmacological Society.
Conflict of interest statement
S.S., A.L., E.Z. and C.N.‐M. are employees of F. Hoffmann‐La Roche Ltd. K.P., R.B. and P.F.S. are employees of Certara and received consultancy fees from Roche for these analyses. L.G. is the owner of QuantPharm LLC and received consultancy fees from Roche for these analyses. S.D. is a former employee of F. Hoffmann‐La Roche Ltd. P.R. is a former employee of F. Hoffman‐La Roche Ltd. and a current employee of Pfizer and hold stocks at F. Hoffman‐La Roche.
Figures


Similar articles
-
Dosing regimen optimisation for oseltamivir in immunocompromised paediatric patients with influenza: Extrapolation of efficacy.Br J Clin Pharmacol. 2022 Mar;88(3):1189-1201. doi: 10.1111/bcp.15059. Epub 2021 Oct 15. Br J Clin Pharmacol. 2022. PMID: 34449090
-
Pharmacokinetic-pharmacodynamic determinants of oseltamivir efficacy using data from phase 2 inoculation studies.Antimicrob Agents Chemother. 2013 Aug;57(8):3478-87. doi: 10.1128/AAC.02440-12. Epub 2013 May 13. Antimicrob Agents Chemother. 2013. PMID: 23669386 Free PMC article. Clinical Trial.
-
Efficacy of oseltamivir treatment started within 5 days of symptom onset to reduce influenza illness duration and virus shedding in an urban setting in Bangladesh: a randomised placebo-controlled trial.Lancet Infect Dis. 2014 Feb;14(2):109-18. doi: 10.1016/S1473-3099(13)70267-6. Epub 2013 Nov 22. Lancet Infect Dis. 2014. PMID: 24268590 Clinical Trial.
-
Oseltamivir: a review of its use in influenza.Drugs. 2001;61(2):263-83. doi: 10.2165/00003495-200161020-00011. Drugs. 2001. PMID: 11270942 Review.
-
Pharmacokinetics and pharmacodynamics of oseltamivir in neonates, infants and children.Infect Disord Drug Targets. 2013 Feb;13(1):6-14. doi: 10.2174/18715265112129990003. Infect Disord Drug Targets. 2013. PMID: 23675922 Review.
Cited by
-
Translation of Pharmacodynamic Biomarkers of Antibiotic Efficacy in Specific Populations to Optimize Doses.Antibiotics (Basel). 2021 Nov 9;10(11):1368. doi: 10.3390/antibiotics10111368. Antibiotics (Basel). 2021. PMID: 34827306 Free PMC article. Review.
-
Influenza and Aging: Clinical Manifestations, Complications, and Treatment Approaches in Older Adults.Drugs Aging. 2025 Jan;42(1):39-55. doi: 10.1007/s40266-024-01169-y. Epub 2025 Jan 7. Drugs Aging. 2025. PMID: 39775605 Review.
References
-
- Ison MG, Hayden FG. Viral infections in immunocompromised patients: what's new with respiratory viruses? Curr Opin Infect Dis. 2002;15(4):355‐367. - PubMed
-
- Ison MG. Influenza, including the novel H1N1, in organ transplant patients. Curr Opin Infect Dis. 2010;23(4):365‐373. - PubMed
-
- Tamiflu (oseltamivir) summary of product characteristics. https://www.ema.europa.eu/en/documents/product-information/tamiflu-epar-.... Accessed January 24, 2020.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
