Diagnostic performance of chest CT in screening patients with suspected COVID-19 infection in a Western population
- PMID: 32808545
- PMCID: PMC7465869
- DOI: 10.1259/bjr.20200643
Diagnostic performance of chest CT in screening patients with suspected COVID-19 infection in a Western population
Abstract
Objective: To investigate the diagnostic performance of chest CT in screening patients suspected of Coronavirus disease 2019 (COVID-19) in a Western population.
Methods: Consecutive patients who underwent chest CT because of clinical suspicion of COVID-19 were included. CT scans were prospectively evaluated by frontline general radiologists who were on duty at the time when the CT scan was performed and retrospectively assessed by a chest radiologist in an independent and blinded manner. Real-time reverse transcriptase-polymerase chain reaction was used as reference standard. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated. Sensitivity and specificity of the frontline general radiologists were compared to those of the chest radiologist using the McNemar test.
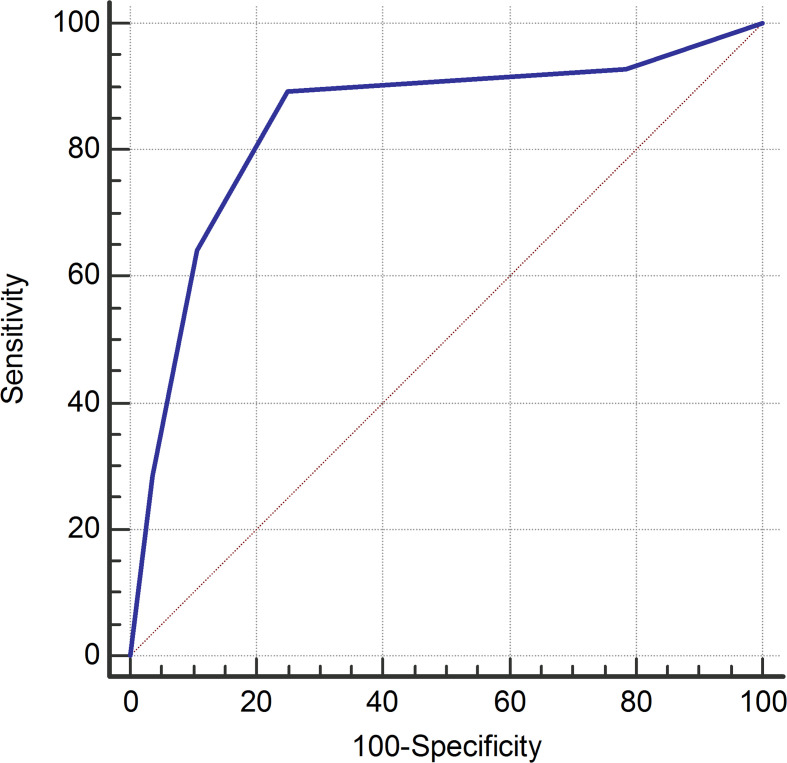
Results: 56 patients were included. Sensitivity, specificity, PPV, and NPV for the frontline general radiologists were 89.3% [95% confidence interval (CI): 71.8%, 97.7%], 32.1% (95% CI: 15.9%, 52.4%), 56.8% (95% CI: 41.0%, 71.7%), and 75.0% (95% CI: 42.8%, 94.5%), respectively. Sensitivity, specificity, PPV, and NPV for the chest radiologist were 89.3% (95% CI: 71.8%, 97.7%), 75.0% (95% CI: 55.1%, 89.3%), 78.1% (95% CI: 60.0%, 90.7%), and 87.5% (95% CI: 67.6%, 97.3%), respectively. Sensitivity was not significantly different (p = 1.000), but specificity was significantly higher for the chest radiologist (p = 0.001).
Conclusion: Chest CT interpreted by frontline general radiologists achieves insufficient screening performance. Although specificity of a chest radiologist appears to be significantly higher, sensitivity did not improve. A negative chest CT result does not exclude COVID-19.
Advances in knowledge: Our study shows that chest CT interpreted by frontline general radiologists achieves insufficient diagnostic performance to use it as an independent screening tool for COVID-19. Although specificity of a chest radiologist appears to be significantly higher, sensitivity is still insufficiently high.
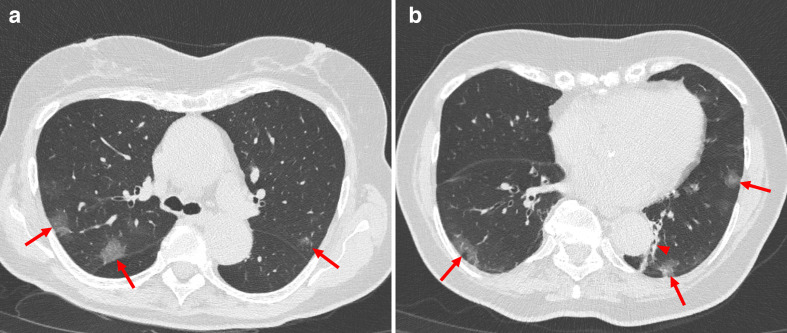
Figures