

Rational surgical neck management in total laryngectomy for advanced stage laryngeal squamous cell carcinomas
- PMID: 32809056
- PMCID: PMC7817600
- DOI: 10.1007/s00432-020-03352-1
Rational surgical neck management in total laryngectomy for advanced stage laryngeal squamous cell carcinomas
Abstract
Purpose: Controversies exist in regard to surgical neck management in total laryngectomies (TL). International guidelines do not sufficiently discriminate neck sides and sublevels, or minimal neck-dissection nodal yield (NY).
Methods: Thirty-seven consecutive primary TL cases from 2009 to 2019 were retrospectively analyzed in terms of local tumor growth using a previously established imaging scheme, metastatic neck involvement, and NY impact on survival.
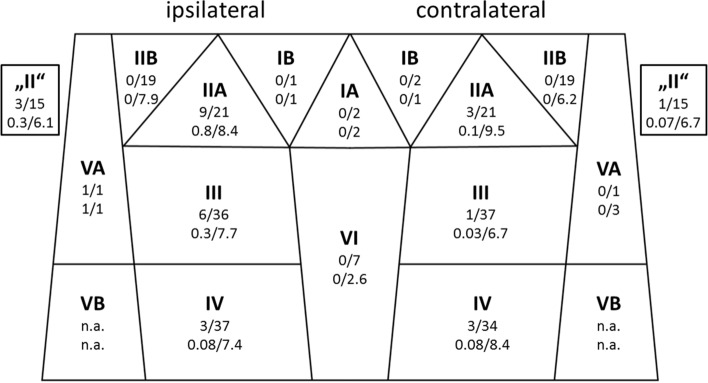
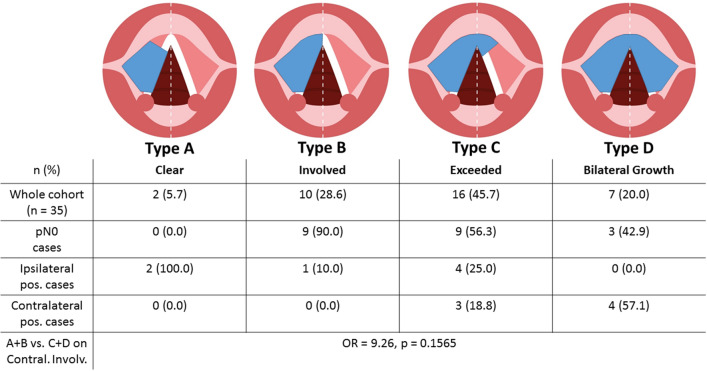
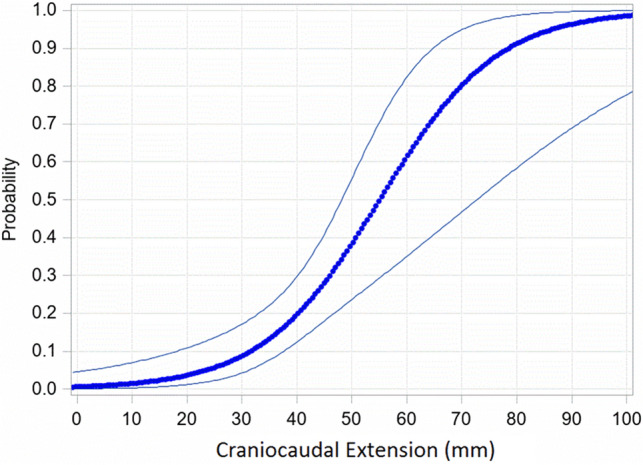
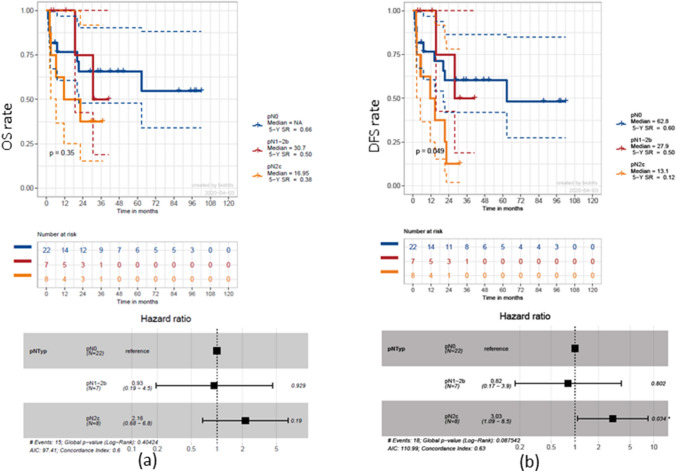
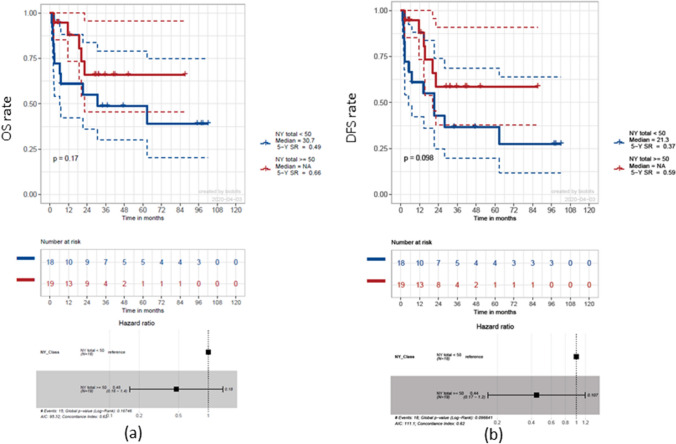
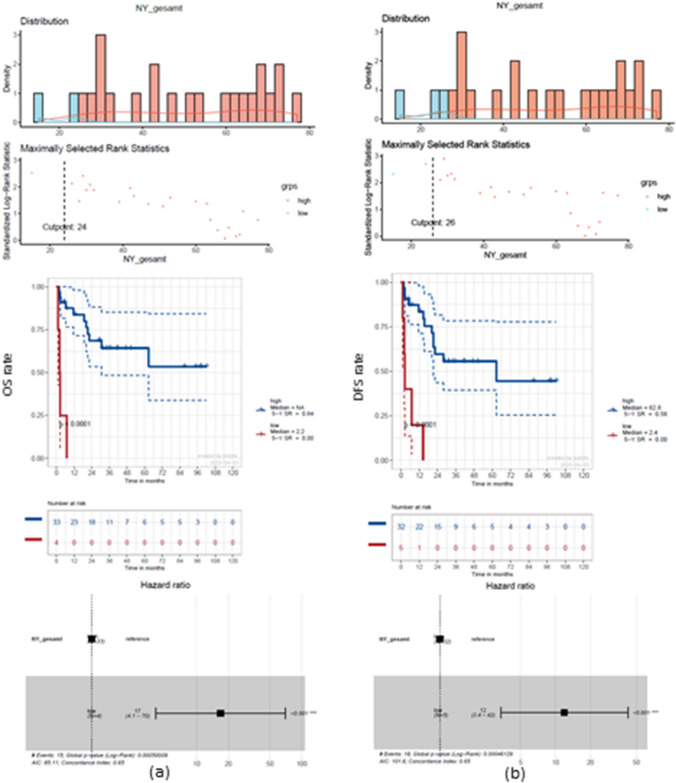
Results: There was no case of level IIB involvement on any side. For type A and B tumor midline involvement, no positive contralateral lymph nodes were found. Craniocaudal tumor extension correlated with contralateral neck involvement (OR: 1.098, p = 0.0493) and showed increased involvement when extending 33 mm (p = 0.0134). Using a bilateral NY of ≥ 24 for 5-year overall survival (OS) and ≥ 26 for 5-year disease-free survival (DFS) gave significantly increased rate advantages of 64 and 56%, respectively (both p < 0.0001).
Conclusions: This work sheds light on regional metastatic distribution pattern and its influence on TL cases. An NY of n ≥ 26 can be considered a desirable benchmark for bilateral selective neck dissections as it leads to improved OS and DFS. Therefore, an omission of distinct neck levels cannot be promoted at this time.
Keywords: Advanced laryngeal cancer; HNSCC; Level IIB; Neck dissection; Nodal yield; Total laryngectomy.
Conflict of interest statement
The other authors declare no conflict of interest.
Figures
References
-
- Balm AJ, Lohuis PJ, Copper MP (2005) Surgical technique–unwrapping the neck node levels around a sternocleidomastoid muscle bar: a systematic way of performing (modified) radical neck dissection. Eur J Surg Oncol 31(10):1216–1221 - PubMed
-
- Böttcher A, Dommerich S, Sander S et al (2016) Nodal yield of neck dissections and influence on outcome in laryngectomized patients. Eur Arch Otorhinolaryngol 273(10):3321–3329 - PubMed
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 68(6):394–424 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
