

Conservative oxygen therapy for mechanically ventilated adults with suspected hypoxic ischaemic encephalopathy
- PMID: 32809136
- PMCID: PMC7431900
- DOI: 10.1007/s00134-020-06196-y
Conservative oxygen therapy for mechanically ventilated adults with suspected hypoxic ischaemic encephalopathy
Abstract
Purpose: Liberal use of oxygen may contribute to secondary brain injury in patients with hypoxic-ischaemic encephalopathy (HIE). However, there are limited data on the effect of different oxygen regimens on survival and neurological disability in HIE patients.
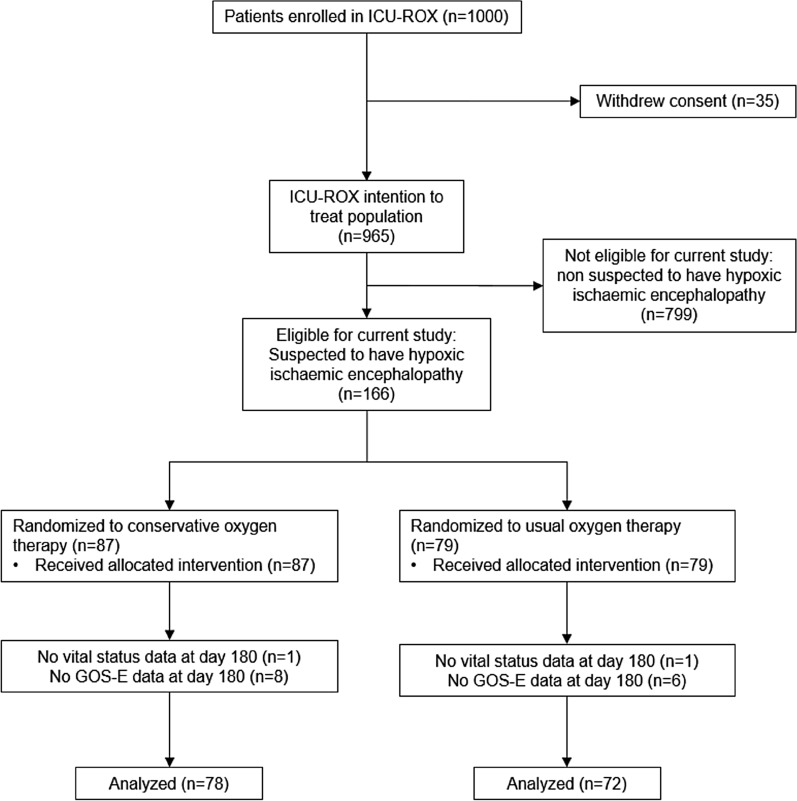
Methods: We undertook a post-hoc analysis of the 166 patients with suspected HIE enrolled in a trial comparing conservative oxygen therapy with usual oxygen therapy in 1000 mechanically ventilated ICU patients. The primary endpoint for the current analysis was death or unfavourable neurological outcome at day 180. Key secondary outcomes were day 180 mortality, and cause-specific mortality.
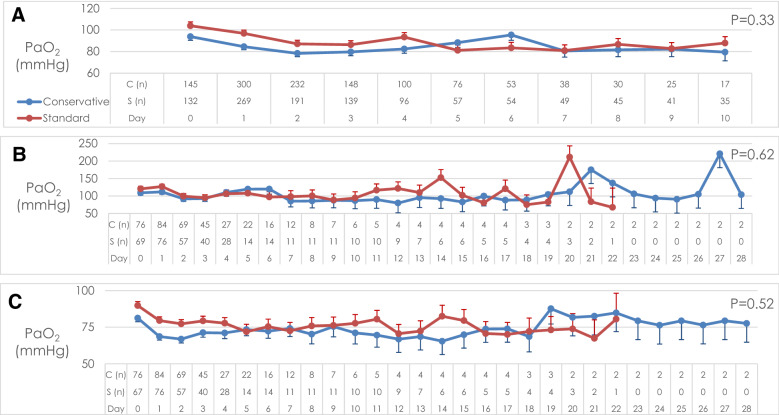
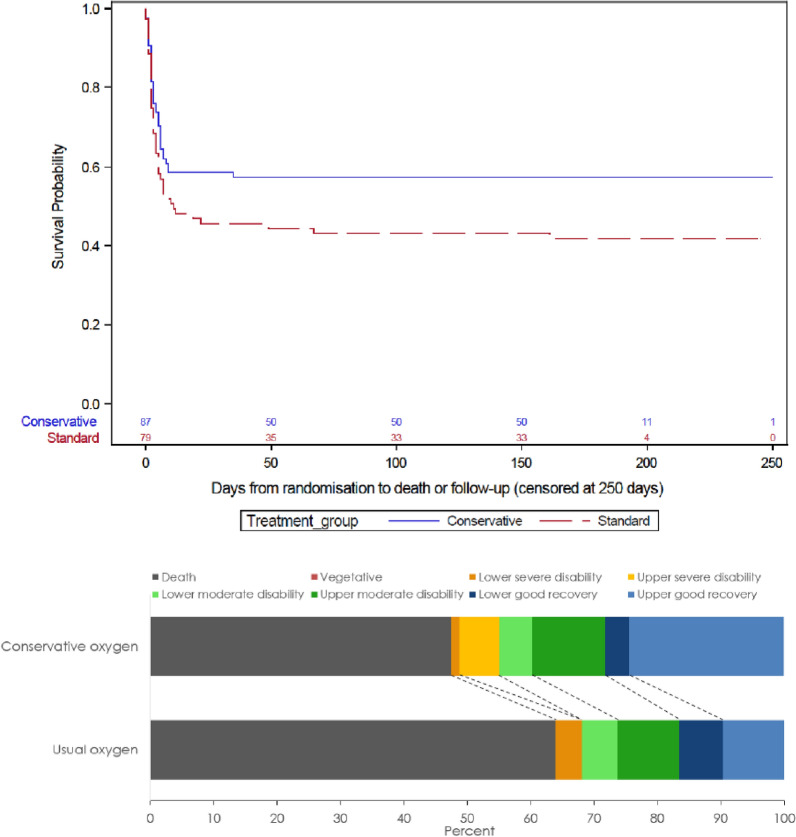
Results: Patients with HIE allocated to conservative oxygen spent less time in the ICU with an SpO2 ≥ 97% (26 h [interquartile range (IQR) 13-45 vs. 35 h [IQR 19-70], absolute difference, 9 h; 95% CI - 21.4 to 3.4). A total of 43 of 78 patients (55.1%) assigned to conservative oxygen and 49 of 72 patients (68.1%) assigned to usual oxygen died or had an unfavourable neurological outcome at day 180; odds ratio 0.58; 95% CI 0.3-1.12; P = 0.1 adjusted odds ratio 0.54; 95% CI 0.23-1.26; P = 0.15. A total of 37 of 86 patients (43%) assigned to conservative oxygen and 46 of 78 (59%) assigned to usual oxygen had died by day 180; odds ratio 0.53; 95% CI 0.28-0.98; P = 0.04; adjusted odds ratio 0.56; 95% CI 0.25-1.23; P = 0.15. Cause-specific mortality was similar by treatment group.
Conclusions: Conservative oxygen therapy was not associated with a statistically significant reduction in death or unfavourable neurological outcomes at day 180. The potential for important benefit or harm from conservative oxygen therapy in HIE patients is not excluded by these data.
Keywords: Cardiac arrest; Critical care; Hypoxic ischemic encephalopathy; Intensive care medicine; Oxygen therapy; Randomized controlled trial.
Conflict of interest statement
Dr. Beasley reports receiving grant support from Fisher and Paykel Healthcare; and Dr. Freebairn, receiving travel support from Hamilton Medical and IMT (Bellavista). No other potential conflict of interest relevant to this article was reported.
Figures
References
-
- Kilgannon JH, Jones AE, Parrillo JE, Dellinger RP, Milcarek B, Hunter K, Shapiro NI, Trzeciak S, Emergency Medicine Shock Research Network Investigators Relationship between supranormal oxygen tension and outcome after resuscitation from cardiac arrest. Circulation. 2011;123:2717–2722. doi: 10.1161/CIRCULATIONAHA.110.001016. - DOI - PubMed
-
- Kilgannon JH, Jones AE, Shapiro NI, Angelos MG, Milcarek B, Hunter K, Parrillo JE, Trzeciak S, Emergency Medicine Shock Research Network Investigators Association between arterial hyperoxia following resuscitation from cardiac arrest and in-hospital mortality. JAMA. 2010;303:2165–2171. doi: 10.1001/jama.2010.707. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
