

The association of standard Kt/V and surface area-normalized standard Kt/V with clinical outcomes in hemodialysis patients
- PMID: 32809268
- PMCID: PMC8006157
- DOI: 10.1111/hdi.12865
The association of standard Kt/V and surface area-normalized standard Kt/V with clinical outcomes in hemodialysis patients
Abstract
Introduction: A previous study demonstrated that the surface area-normalized standard Kt/V (SAstdKt/V) was better associated with mortality than standard Kt/V (stdKt/V). This study investigates the association of SAstdKt/V and stdKt/V with mortality, anemia, and hypoalbuminemia in a larger patient cohort with a longer follow-up period.
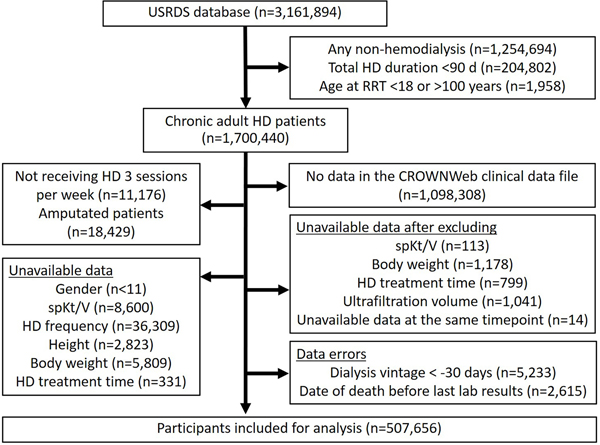
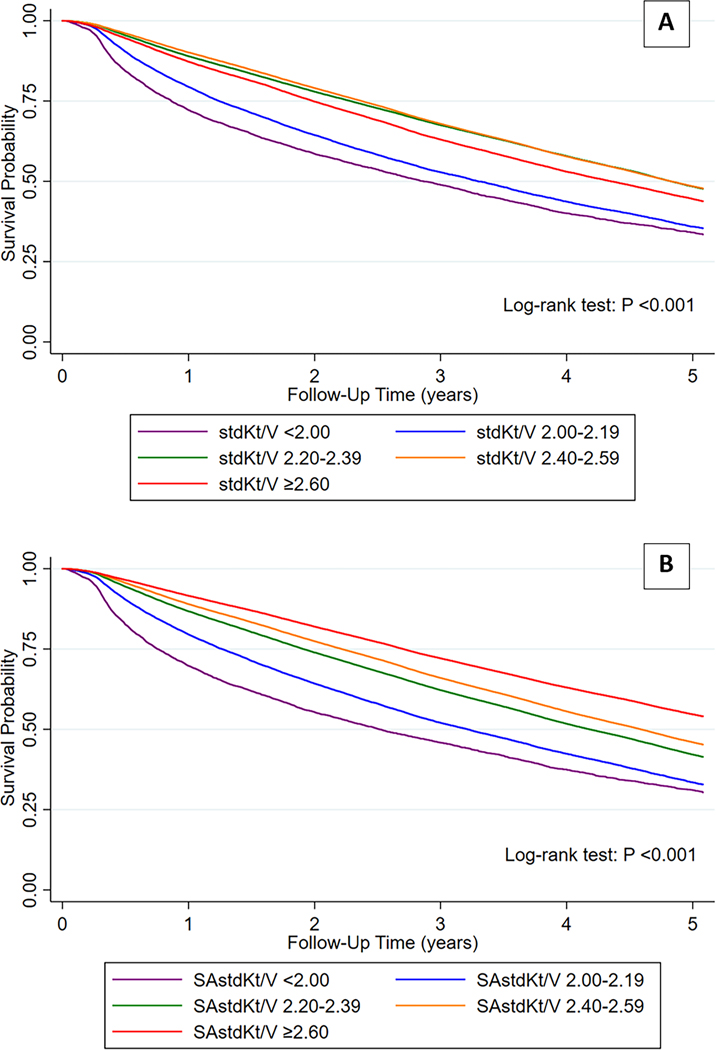
Methods: We included adult patients on thrice-weekly hemodialysis in the USRDS database and excluded amputated patients. StdKt/V and SAstdKt/V were calculated from the available single-pool Kt/V. Patients were categorized into five groups according to their stdKt/V and SAstdKt/V: <2.00, 2.00-2.19, 2.20-2.39, 2.40-2.59, and ≥2.60. Hazard ratios (HR) and odds ratios (OR) were calculated using Cox and logistic regression analysis respectively.
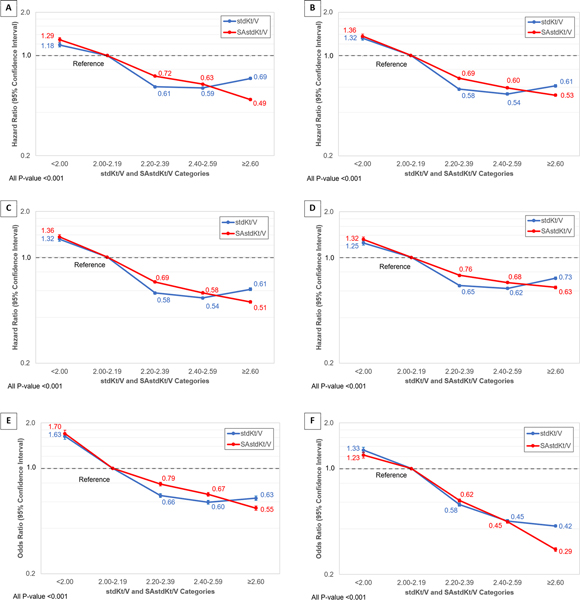
Findings: There were 507,656 patients included in the analysis. The patients had a median age of 65.5 years with a median follow-up period of 2 years. Thirty-four percent died during follow-up. HRs for mortality progressively decreased as SAstdKt/V increased in both unadjusted and adjusted models. Unlike SAstdKt/V, HRs were the lowest in the categories with stdKt/V of 2.40-2.59 and they increased in the higher stdKt/V category. The adjusted HR for SAstdKt/V vs. stdKt/V were 0.68 vs. 0.62 in the category of 2.40-2.59, and 0.63 vs. 0.73 in the category of ≥2.60. The adjusted ORs for anemia progressively decreased as SAstdKt/V increased, whereas ORs decreased to the lowest in stdKt/V category 2.40-2.59 and increased in the ≥2.60 category. The adjusted ORs for hypoalbuminemia progressively decreased as SAstdKt/V and stdKt/V increased which were both 0.45 in 2.40-2.59 category and decreased to 0.29 and 0.42 in the ≥2.60 category.
Discussion: SAstdKt/V is better associated with mortality, anemia, and hypoalbuminemia than stdKt/V. SAstdKt/V is a better parameter in defining hemodialysis dosing which can be calculated by an available online tool. Further studies to determine the optimal SAstdKt/V dose required to achieve improved clinical outcomes with better cost-effectiveness are needed.
Keywords: Adequacy of dialysis; anemia; nutrition; survival.
© 2020 International Society for Hemodialysis.
Conflict of interest statement
Conflict of Interest Statement
Other authors declare that they have no conflict of interest.
Figures
Similar articles
-
Dialysis dose scaled to body surface area and size-adjusted, sex-specific patient mortality.Clin J Am Soc Nephrol. 2012 Dec;7(12):1977-87. doi: 10.2215/CJN.00390112. Epub 2012 Sep 13. Clin J Am Soc Nephrol. 2012. PMID: 22977208 Free PMC article.
-
Surface-area-normalized Kt/V: a method of rescaling dialysis dose to body surface area-implications for different-size patients by gender.Semin Dial. 2008 Sep-Oct;21(5):415-21. doi: 10.1111/j.1525-139X.2008.00482.x. Semin Dial. 2008. PMID: 18945330 Free PMC article.
-
Predicting treatment dose for novel therapies using urea standard Kt/V.Semin Dial. 2004 Mar-Apr;17(2):142-5. doi: 10.1111/j.0894-0959.2004.17212.x. Semin Dial. 2004. PMID: 15043617
-
Is Hemodialysis Patient Survival Dependent upon Small Solute Clearance (Kt/V)?: If So How Can Kt/V be Adjusted to Prevent Under Dialysis in Vulnerable Groups?Semin Dial. 2017 Mar;30(2):86-92. doi: 10.1111/sdi.12566. Epub 2017 Jan 11. Semin Dial. 2017. PMID: 28074616 Review.
-
Adequacy in dialysis: intermittent versus continuous therapies.Nefrologia. 2000;20 Suppl 3:25-32. Nefrologia. 2000. PMID: 10835874 Review.
Cited by
-
Correlation between β2-microglobulin level and risk of cardiovascular events and prognosis in hemodialysis patients.Am J Transl Res. 2025 Feb 15;17(2):1428-1436. doi: 10.62347/FLPF7627. eCollection 2025. Am J Transl Res. 2025. PMID: 40092135 Free PMC article.
-
Korean Society of Nephrology 2021 Clinical Practice Guideline for Optimal Hemodialysis Treatment.Kidney Res Clin Pract. 2021 Dec;40(Suppl 1):S1-S37. doi: 10.23876/j.krcp.21.600. Epub 2021 Dec 10. Kidney Res Clin Pract. 2021. PMID: 34923803 Free PMC article. No abstract available.
-
Clinical Outcomes in Patients on Hemodialysis with Congestive Heart Failure.Kidney Dis (Basel). 2023 Mar 3;9(4):306-316. doi: 10.1159/000529802. eCollection 2023 Aug. Kidney Dis (Basel). 2023. PMID: 37900002 Free PMC article.
References
-
- Daugirdas JT, Depner TA, Inrig J, et al. KDOQI Clinical Practice Guideline for Hemodialysis Adequacy: 2015 Update. Am J Kidney Dis 2015; 66: 884–930. - PubMed
-
- Gotch FA, Sargent JA. A mechanistic analysis of the National Cooperative Dialysis Study (NCDS). Kidney Int 1985; 28: 526–534. - PubMed
-
- Held PJ, Port FK, Wolfe RA, et al. The dose of hemodialysis and patient mortality. Kidney Int 1996; 50: 550–556. - PubMed
-
- Eknoyan G, Beck GJ, Cheung AK, et al. Effect of dialysis dose and membrane flux in maintenance hemodialysis. N Engl J Med 2002; 347: 2010–2019. - PubMed
-
- Depner T, Daugirdas J, Greene TOM, et al. Dialysis dose and the effect of gender and body size on outcome in the HEMO Study. Kidney Int 2004; 65: 1386–1394. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
